

Kidney Function Decline and Apparent Treatment-Resistant Hypertension in the Elderly
- PMID: 26807712
- PMCID: PMC4726557
- DOI: 10.1371/journal.pone.0146056
Kidney Function Decline and Apparent Treatment-Resistant Hypertension in the Elderly
Abstract
Background: Cross-sectional studies show a strong association between chronic kidney disease and apparent treatment-resistant hypertension, but the longitudinal association of the rate of kidney function decline with the risk of resistant hypertension is unknown.
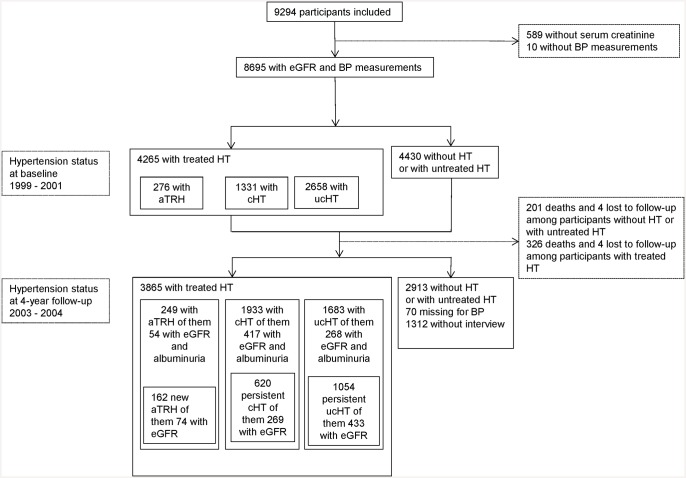
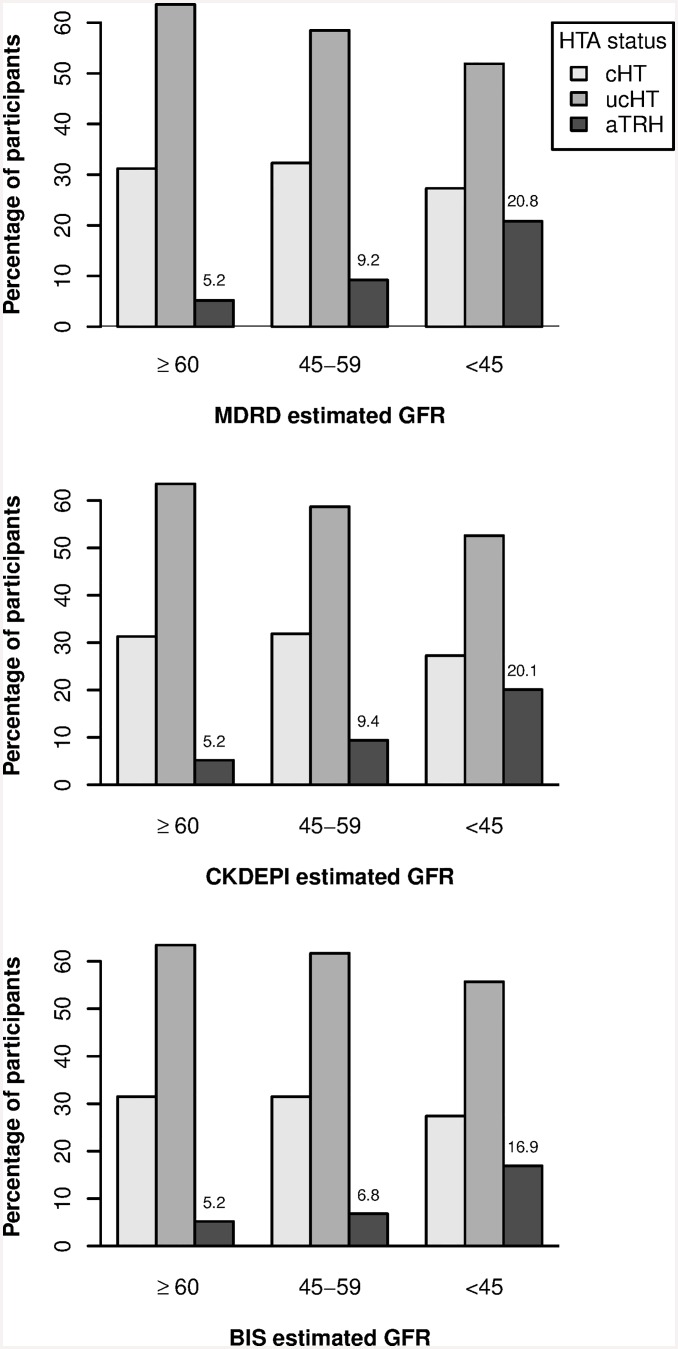
Methods: The population-based Three-City included 8,695 participants older than 65 years, 4265 of them treated for hypertension. We estimated the odds ratios (OR) of new-onset apparent treatment-resistant hypertension, defined as blood pressure ≥ 140/90 mmHg despite use of 3 antihypertensive drug classes or ≥ 4 classes regardless of blood pressure, associated with the mean estimated glomerular filtration rate (eGFR) level and its rate of decline over 4 years, compared with both controlled hypertension and uncontrolled nonresistant hypertension with ≤ 2 drugs. GFR was estimated with three different equations.
Results: Baseline prevalence of apparent treatment-resistant hypertension and of controlled and uncontrolled nonresistant hypertension, were 6.5%, 62.3% and 31.2%, respectively. During follow-up, 162 participants developed apparent treatment-resistant hypertension. Mean eGFR decline with the MDRD equation was 1.5±2.9 mL/min/1.73 m² per year: 27.7% of the participants had an eGFR ≥3 and 10.1% ≥ 5 mL/min/1.73 m² per year. After adjusting for age, sex, obesity, diabetes, and cardiovascular history, the ORs for new-onset apparent treatment-resistant hypertension associated with a mean eGFR level, per 15 mL/min/1.73 m² drop, were 1.23 [95% confidence interval 0.91-1.64] compared to controlled hypertension and 1.10 [0.83-1.45] compared to uncontrolled nonresistant hypertension; ORs associated with a decline rate ≥ 3 mL/min/1.73 m² per year were 1.89 [1.09-3.29] and 1.99 [1.19-3.35], respectively. Similar results were obtained when we estimated GFR with the CKDEPI and the BIS1 equations. ORs tended to be higher for an eGFR decline rate ≥ 5 mL/min/1.73 m² per year.
Conclusion: The speed of kidney function decline is associated more strongly than kidney function itself with the risk of apparent treatment-resistant hypertension in the elderly.
Conflict of interest statement
Figures
Similar articles
-
Prevalence of apparent treatment-resistant hypertension among individuals with CKD.Clin J Am Soc Nephrol. 2013 Sep;8(9):1583-90. doi: 10.2215/CJN.00550113. Epub 2013 Jul 18. Clin J Am Soc Nephrol. 2013. PMID: 23868902 Free PMC article.
-
Resistant Hypertension, Time-Updated Blood Pressure Values and Renal Outcome in Type 2 Diabetes Mellitus.J Am Heart Assoc. 2017 Sep 22;6(9):e006745. doi: 10.1161/JAHA.117.006745. J Am Heart Assoc. 2017. PMID: 28939716 Free PMC article.
-
Prevalence and risk factors of chronic kidney disease in urban adult Cameroonians according to three common estimators of the glomerular filtration rate: a cross-sectional study.BMC Nephrol. 2015 Jul 7;16:96. doi: 10.1186/s12882-015-0102-9. BMC Nephrol. 2015. PMID: 26149764 Free PMC article.
-
Extracellular Fluid Volume Is an Independent Determinant of Uncontrolled and Resistant Hypertension in Chronic Kidney Disease: A NephroTest Cohort Study.J Am Heart Assoc. 2018 Oct 2;7(19):e010278. doi: 10.1161/JAHA.118.010278. J Am Heart Assoc. 2018. PMID: 30371309 Free PMC article.
-
Resistant and Apparently Resistant Hypertension in Peritoneally Dialyzed Patients.J Clin Med. 2025 Jan 2;14(1):218. doi: 10.3390/jcm14010218. J Clin Med. 2025. PMID: 39797299 Free PMC article. Review.
Cited by
-
Hypertension Control, Apparent Treatment Resistance, and Outcomes in the Elderly Population With Chronic Kidney Disease.Kidney Int Rep. 2016 Oct 31;2(2):180-191. doi: 10.1016/j.ekir.2016.10.006. eCollection 2017 Mar. Kidney Int Rep. 2016. PMID: 29142956 Free PMC article.
-
Persistent Resistant Hypertension Has Worse Renal Outcomes in Chronic Kidney Disease than that Resolved in Two Years: Results from the KNOW-CKD Study.J Clin Med. 2021 Sep 3;10(17):3998. doi: 10.3390/jcm10173998. J Clin Med. 2021. PMID: 34501446 Free PMC article.
-
MR-SPLIT: A novel method to address selection and weak instrument bias in one-sample Mendelian randomization studies.PLoS Genet. 2024 Sep 6;20(9):e1011391. doi: 10.1371/journal.pgen.1011391. eCollection 2024 Sep. PLoS Genet. 2024. PMID: 39241053 Free PMC article.
-
Selecting Transfemoral Access or Upper Extremity Access for Renal Denervation Based on Vascular Morphology: Long-term Results.J Clin Hypertens (Greenwich). 2024 Dec;26(12):1513-1520. doi: 10.1111/jch.14937. Epub 2024 Nov 17. J Clin Hypertens (Greenwich). 2024. PMID: 39552183 Free PMC article.
-
The renal molecular clock: broken by aging and restored by exercise.Am J Physiol Renal Physiol. 2019 Nov 1;317(5):F1087-F1093. doi: 10.1152/ajprenal.00301.2019. Epub 2019 Aug 28. Am J Physiol Renal Physiol. 2019. PMID: 31461350 Free PMC article. Review.
References
-
- Peralta CA, Norris KC, Li S, Chang TI, Tamura MK, Jolly SE, et al. Blood pressure components and end-stage renal disease in persons with chronic kidney disease: the Kidney Early Evaluation Program (KEEP). Arch Intern Med. 2012. January 9;172(1):41–7. 10.1001/archinternmed.2011.619 - DOI - PMC - PubMed
-
- Tonelli M, Gill J, Pandeya S, Bohm C, Levin A, Kiberd BA. Barriers to blood pressure control and angiotensin enzyme inhibitor use in Canadian patients with chronic renal insufficiency. Nephrol Dial Transplant. 2002;17(March 2000):1426–33. - PubMed
-
- Iyer AS, Ahmed MI, Filippatos GS, Ekundayo OJ, Aban IB, Love TE, et al. Uncontrolled hypertension and increased risk for incident heart failure in older adults with hypertension: findings from a propensity-matched prospective population study. J Am Soc Hypertens. Elsevier Ltd; 2010;4(1):22–31. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
