

Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis
- PMID: 26808317
- PMCID: PMC4725677
- DOI: 10.1371/journal.pone.0147601
Panethnic Differences in Blood Pressure in Europe: A Systematic Review and Meta-Analysis
Abstract
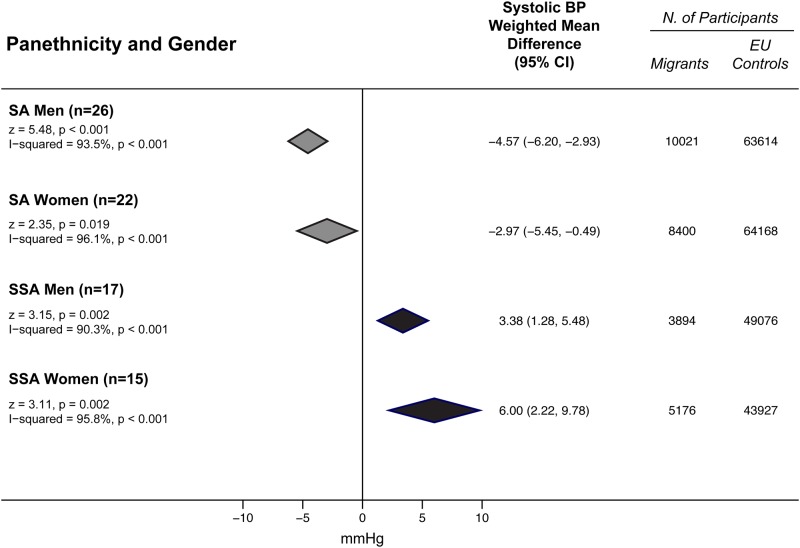
Background: People of Sub Saharan Africa (SSA) and South Asians(SA) ethnic minorities living in Europe have higher risk of stroke than native Europeans(EU). Study objective is to provide an assessment of gender specific absolute differences in office systolic(SBP) and diastolic(DBP) blood pressure(BP) levels between SSA, SA, and EU.
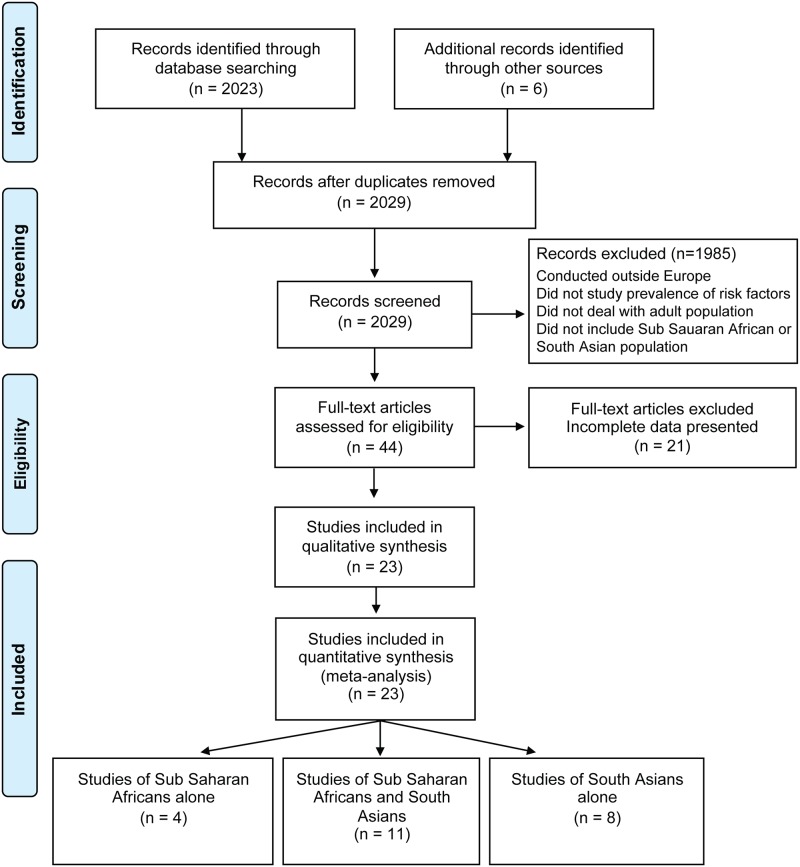
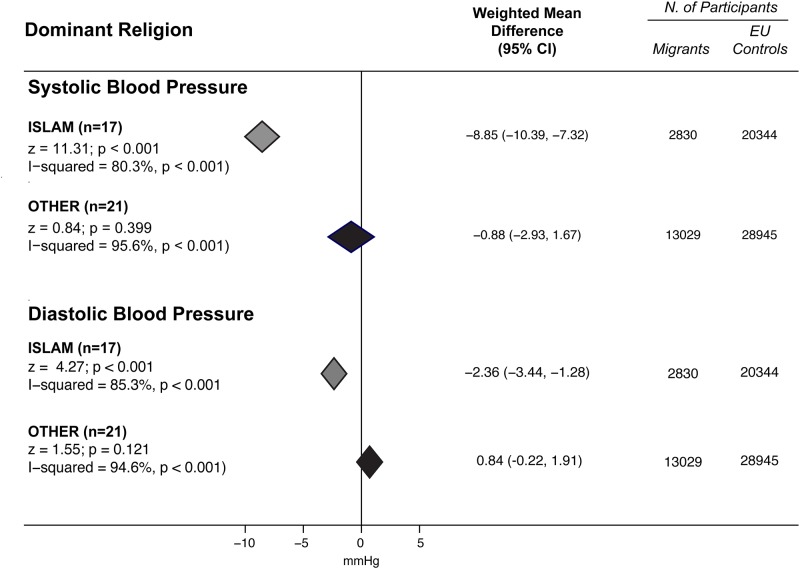
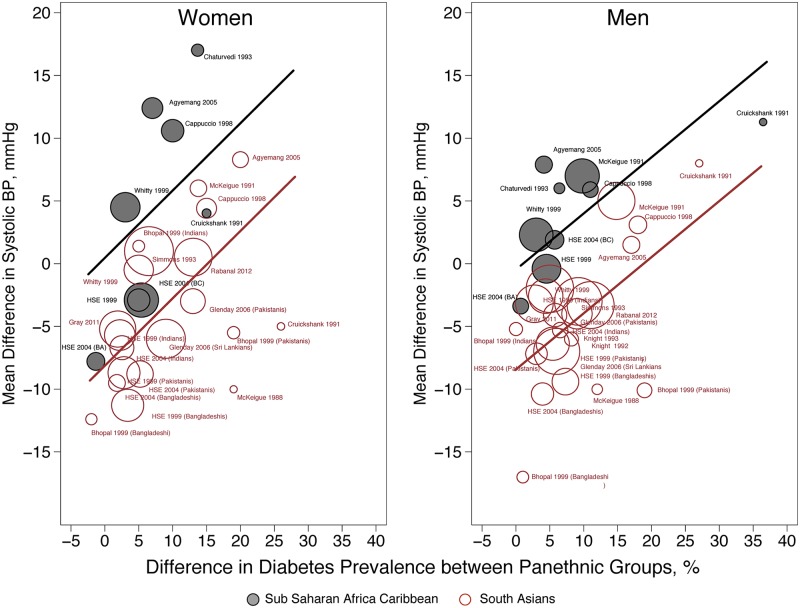
Methods and findings: We performed a systematic review and meta-analysis of observational studies conducted in Europe that examined BP in non-selected adult SSA, SA and EU subjects. Medline, PubMed, Embase, Web of Science, and Scopus were searched from their inception through January 31st 2015, for relevant articles. Outcome measures were mean SBP and DBP differences between minorities and EU, using a random effects model and tested for heterogeneity. Twenty-one studies involving 9,070 SSA, 18,421 SA, and 130,380 EU were included. Compared with EU, SSA had higher values of both SBP (3.38 mmHg, 95% CI 1.28 to 5.48 mmHg; and 6.00 mmHg, 95% CI 2.22 to 9.78 in men and women respectively) and DBP (3.29 mmHg, 95% CI 1.80 to 4.78; 5.35 mmHg, 95% CI 3.04 to 7.66). SA had lower SBP than EU(-4.57 mmHg, 95% CI -6.20 to -2.93; -2.97 mmHg, 95% CI -5.45 to -0.49) but similar DBP values. Meta-analysis by subgroup showed that SA originating from countries where Islam is the main religion had lower SBP and DBP values than EU. In multivariate meta-regression analyses, SBP difference between minorities and EU populations, was influenced by panethnicity and diabetes prevalence.
Conclusions: 1) The higher BP in SSA is maintained over decades, suggesting limited efficacy of prevention strategies in such group in Europe;2) The lower BP in Muslim populations suggests that yet untapped lifestyle and behavioral habits may reveal advantages towards the development of hypertension;3) The additive effect of diabetes, emphasizes the need of new strategies for the control of hypertension in groups at high prevalence of diabetes.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
