

Patient injuries in primary total hip replacement
- PMID: 26808350
- PMCID: PMC4900093
- DOI: 10.3109/17453674.2015.1135662
Patient injuries in primary total hip replacement
Abstract
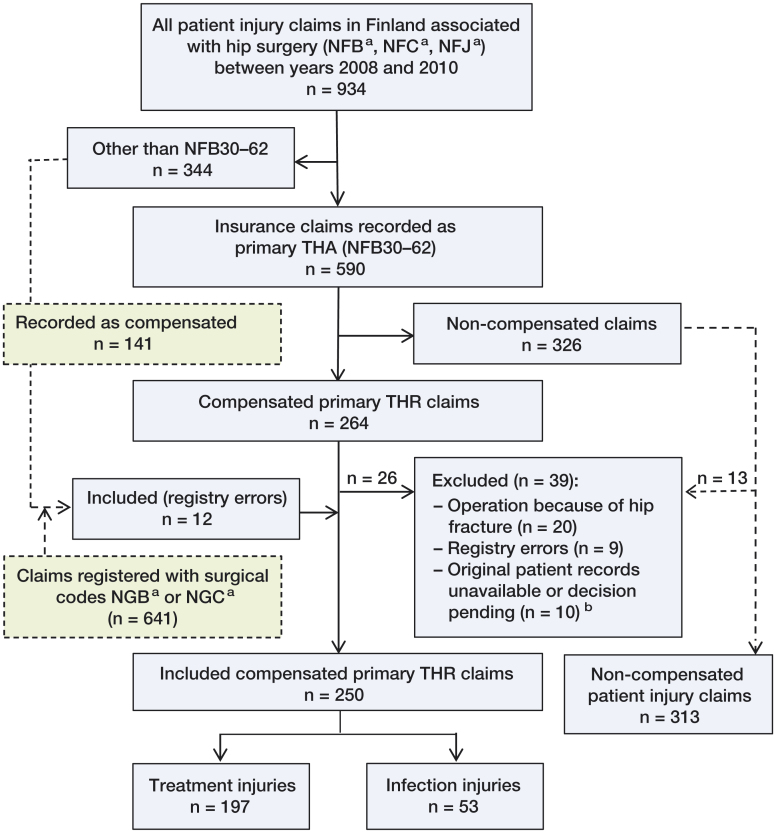
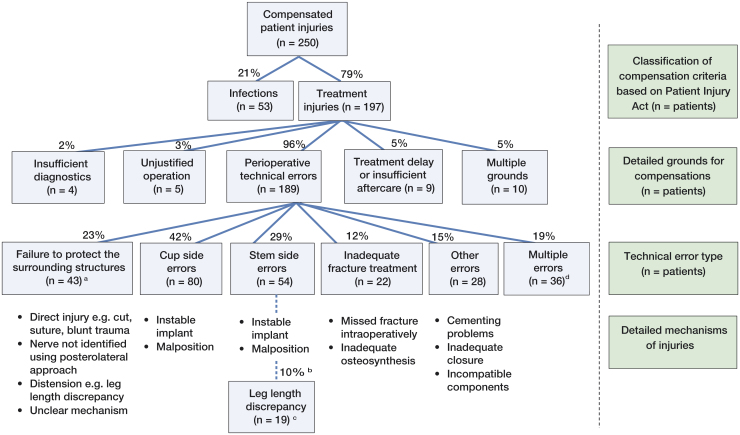
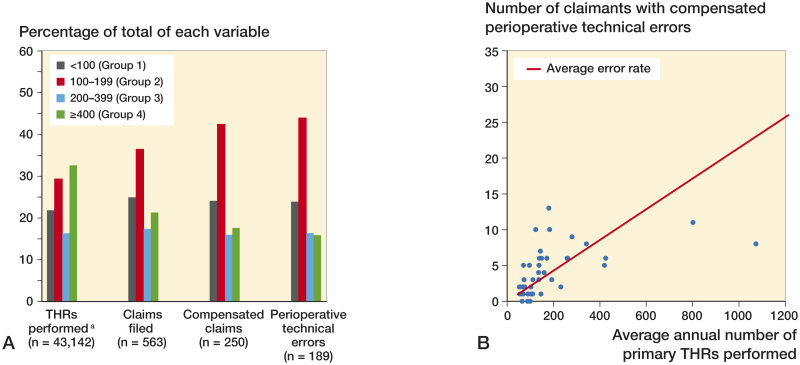
Background and purpose - Although the results of primary total hip replacements (THRs) are generally excellent, sometimes serious complications arise. Some of these severe complications are considered to be patient injuries. We analyzed primary THR-related patient injuries in a nationwide setting. Patients and methods - We evaluated all the primary THR-related patient injury claims in Finland between 2008 and 2010. We used the original medical records and 2 nationwide registries, the Care Register for Social Welfare and Health Care and the Patient Injury Claim Register. Results - We identified 563 claims, 44% of which were compensated (n = 250). Of these 250 compensated claims, 79% were considered to be avoidable (treatment injuries) and 21% were severe unexpected infections (with a preoperative infection risk of less than 2%). The most common type of technical error was cup malposition (31%). High-volume hospitals (with an annual primary THR volume ≥ 400) had a lower patient injury rate. In lower-volume hospitals (with an annual primary THR volume of < 400), the relative risks (RRs) of patient injury for any reason, due to technical errors, or because of cup malposition were 2-fold (95% CI: 1.6-3.1), 4-fold (95% CI: 2.3-6.2), and 9-fold (95% CI: 3-28), respectively, compared to high-volume hospitals. Interpretation - Our study provides the first comprehensive nationwide data on THR-related patient injury types. Hospital volume was associated with the quality and quantity of errors detected. An annual hospital volume of ≥ 400 primary THRs was established as a protective factor against patient injuries.
Figures
Comment on
-
Relationship between the volume of total hip replacements performed by providers and the rates of postoperative complications in the state of Washington.J Bone Joint Surg Am. 1997 Apr;79(4):485-94. doi: 10.2106/00004623-199704000-00003. J Bone Joint Surg Am. 1997. PMID: 9111392
-
The effect of hospital volume on the in-hospital complication rate in knee replacement patients.Health Serv Res. 1998 Dec;33(5 Pt 1):1191-210. Health Serv Res. 1998. PMID: 9865217 Free PMC article.
-
The Frank Stinchfield Award. Sudden death during primary hip arthroplasty.Clin Orthop Relat Res. 1999 Dec;(369):39-48. doi: 10.1097/00003086-199912000-00005. Clin Orthop Relat Res. 1999. PMID: 10611859
-
Negligent care and malpractice claiming behavior in Utah and Colorado.Med Care. 2000 Mar;38(3):250-60. doi: 10.1097/00005650-200003000-00002. Med Care. 2000. PMID: 10718350
-
Thirty-day mortality after elective total hip arthroplasty.J Bone Joint Surg Am. 2001 Oct;83(10):1524-8. doi: 10.2106/00004623-200110000-00010. J Bone Joint Surg Am. 2001. PMID: 11679603
-
Association between hospital and surgeon procedure volume and outcomes of total hip replacement in the United States medicare population.J Bone Joint Surg Am. 2001 Nov;83(11):1622-9. doi: 10.2106/00004623-200111000-00002. J Bone Joint Surg Am. 2001. PMID: 11701783
-
The Swedish Total Hip Replacement Register.J Bone Joint Surg Am. 2002;84-A Suppl 2:2-20. doi: 10.2106/00004623-200200002-00002. J Bone Joint Surg Am. 2002. PMID: 12479335 No abstract available.
-
Do women simply complain more? National patient injury claims data show gender and age differences.Qual Manag Health Care. 2003 Oct-Dec;12(4):225-31. doi: 10.1097/00019514-200310000-00007. Qual Manag Health Care. 2003. PMID: 14603784
-
A prospective, randomised, controlled trial of the use of drains in total hip arthroplasty.J Bone Joint Surg Br. 2005 Oct;87(10):1397-401. doi: 10.1302/0301-620X.87B10.16221. J Bone Joint Surg Br. 2005. PMID: 16189315 Clinical Trial.
-
Increased surgical volume is associated with lower THA dislocation rates.Clin Orthop Relat Res. 2006 Jun;447:28-33. doi: 10.1097/01.blo.0000218743.99741.f0. Clin Orthop Relat Res. 2006. PMID: 16672898 Review.
-
An analysis of the risk of hip dislocation with a contemporary total joint registry.Clin Orthop Relat Res. 2006 Jun;447:19-23. doi: 10.1097/01.blo.0000218752.22613.78. Clin Orthop Relat Res. 2006. PMID: 16741469
-
Claiming behaviour in a no-fault system of medical injury: a descriptive analysis of claimants and non-claimants.Med J Aust. 2006 Aug 21;185(4):203-7. doi: 10.5694/j.1326-5377.2006.tb00532.x. Med J Aust. 2006. PMID: 16922665
-
Total joint arthroplasty: When do fatal or near-fatal complications occur?J Bone Joint Surg Am. 2007 Jan;89(1):27-32. doi: 10.2106/JBJS.E.01443. J Bone Joint Surg Am. 2007. PMID: 17200306
-
Patterns of technical error among surgical malpractice claims: an analysis of strategies to prevent injury to surgical patients.Ann Surg. 2007 Nov;246(5):705-11. doi: 10.1097/SLA.0b013e31815865f8. Ann Surg. 2007. PMID: 17968158
-
High-volume surgeons in regard to reductions in operating time, blood loss, and postoperative complications for total hip arthroplasty.J Orthop Sci. 2009 Jan;14(1):3-9. doi: 10.1007/s00776-008-1289-4. Epub 2009 Feb 13. J Orthop Sci. 2009. PMID: 19214681
-
Monitoring surgical performance: an application to total hip replacement.J Eval Clin Pract. 2009 Jun;15(3):420-4. doi: 10.1111/j.1365-2753.2008.01029.x. Epub 2009 Apr 2. J Eval Clin Pract. 2009. PMID: 19366396
-
Shoulder arthroplasties have fewer complications than hip or knee arthroplasties in US veterans.Clin Orthop Relat Res. 2010 Mar;468(3):717-22. doi: 10.1007/s11999-009-0996-2. Epub 2009 Jul 21. Clin Orthop Relat Res. 2010. PMID: 19626383 Free PMC article.
-
Monitoring the quality of total hip replacement in a tertiary care department using a cumulative summation statistical method (CUSUM).J Bone Joint Surg Br. 2011 Sep;93(9):1183-8. doi: 10.1302/0301-620X.93B9.26436. J Bone Joint Surg Br. 2011. PMID: 21911528
-
Factors predisposing to claims and compensations for patient injuries following total hip and knee arthroplasty.Acta Orthop. 2012 Apr;83(2):190-6. doi: 10.3109/17453674.2012.672089. Epub 2012 Mar 8. Acta Orthop. 2012. PMID: 22401679 Free PMC article.
-
Adverse outcomes in hip arthroplasty: long-term trends.J Bone Joint Surg Am. 2012 Jul 18;94(14):e103. doi: 10.2106/JBJS.K.00011. J Bone Joint Surg Am. 2012. PMID: 22810410 Free PMC article.
-
Risk factors associated with surgical site infection in 30,491 primary total hip replacements.J Bone Joint Surg Br. 2012 Oct;94(10):1330-8. doi: 10.1302/0301-620X.94B10.29184. J Bone Joint Surg Br. 2012. PMID: 23015556
-
Lessons regarding the safety of orthopaedic patient care: an analysis of four hundred and sixty-four closed malpractice claims.J Bone Joint Surg Am. 2013 Feb 20;95(4):e201-8. doi: 10.2106/JBJS.K.01272. J Bone Joint Surg Am. 2013. PMID: 23426777
-
Learning curve of acetabular cup positioning in total hip arthroplasty using a cumulative summation test for learning curve (LC-CUSUM).J Arthroplasty. 2014 Mar;29(3):586-9. doi: 10.1016/j.arth.2013.07.023. Epub 2013 Aug 30. J Arthroplasty. 2014. PMID: 23998991
-
Accuracy of acetabular component position in hip arthroplasty.J Bone Joint Surg Am. 2013 Oct 2;95(19):1760-8. doi: 10.2106/JBJS.L.01704. J Bone Joint Surg Am. 2013. PMID: 24088968
-
Relation between surgeon volume and risk of complications after total hip arthroplasty: propensity score matched cohort study.BMJ. 2014 May 23;348:g3284. doi: 10.1136/bmj.g3284. BMJ. 2014. PMID: 24859902 Free PMC article.
References
-
- Barrack R L, Krempec J A, Clohisy J C, McDonald D J, Ricci W M, Ruh E L, Nunley R M.. Accuracy of acetabular component position in hip artroplasty. J Bone Joint Surg (Am) 2013; 95: 1760–8. - PubMed
-
- Battaglia T C, Mulhall K J, Brown T E, Saleh K J.. Increased surgical volume is associated with lower THR dislocation rates. Clin Orthop Relat Res 2006; 447: 28–33. Review. - PubMed
-
- Bender R. Calculating confidence intervals for the number needed to treat. Control Clin Trials 2001; 22(2): 102–10. - PubMed
-
- Biau D J, Milet A, Thévenin F, Anract P, Porcher R.. Monitoring surgical performance: an application to total hip replacement. J Eval Clin Pract 2009; 15(3): 420–4. - PubMed
-
- Biau D J, Meziane M, Bhumbra R S, Dumaine V, Babinet A, Anract P.. Monitoring the quality of total hip replacement in a tertiary care department using a cumulative summation statistical method (CUSUM). J Bone Joint Surg (Br) 2011; 93(9): 1183–8. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical