

The Spread of Dengue in an Endemic Urban Milieu--The Case of Delhi, India
- PMID: 26808518
- PMCID: PMC4726601
- DOI: 10.1371/journal.pone.0146539
The Spread of Dengue in an Endemic Urban Milieu--The Case of Delhi, India
Erratum in
-
Correction: The Spread of Dengue in an Endemic Urban Milieu-The Case of Delhi, India.PLoS One. 2016 Mar 29;11(3):e0152847. doi: 10.1371/journal.pone.0152847. eCollection 2016. PLoS One. 2016. PMID: 27023753 Free PMC article. No abstract available.
Abstract
Background: Dengue is a major international public health concern, one of the most important arthropod-borne diseases. More than 3.5 billion people are at risk of dengue infection and there are an estimated 390 million dengue infections annually. This prolific increase has been connected to societal changes such as population growth and increasing urbanization generating intense agglomeration leading to proliferation of synanthropic mosquito species. Quantifying the spatio-temporal epidemiology of dengue in large cities within the context of a Geographic Information System is a first step in the identification of socio-economic risk factors.
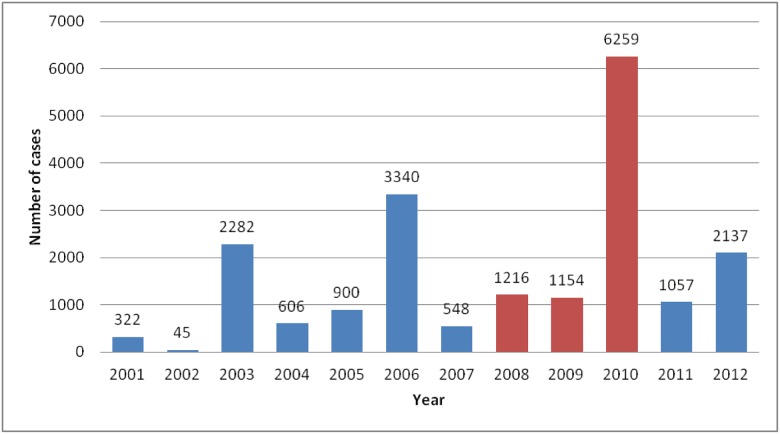
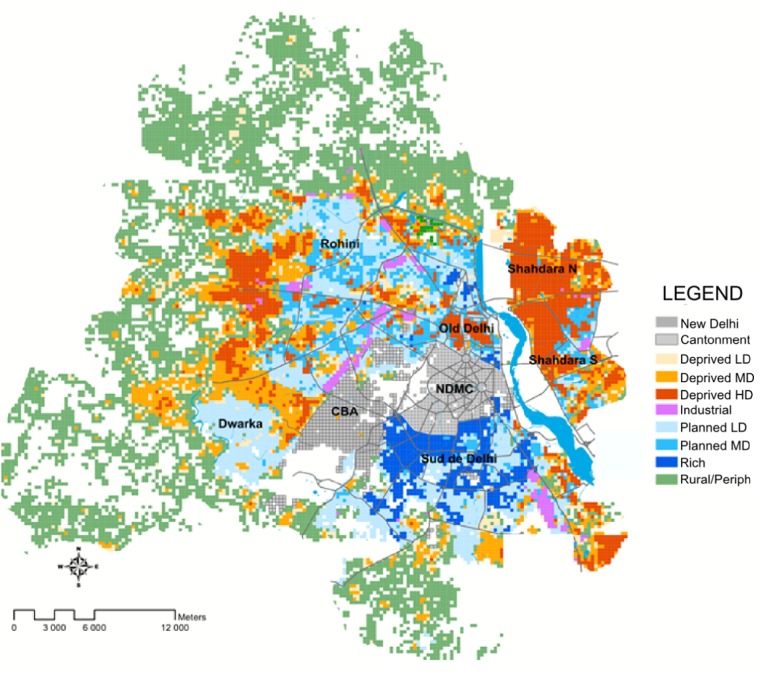
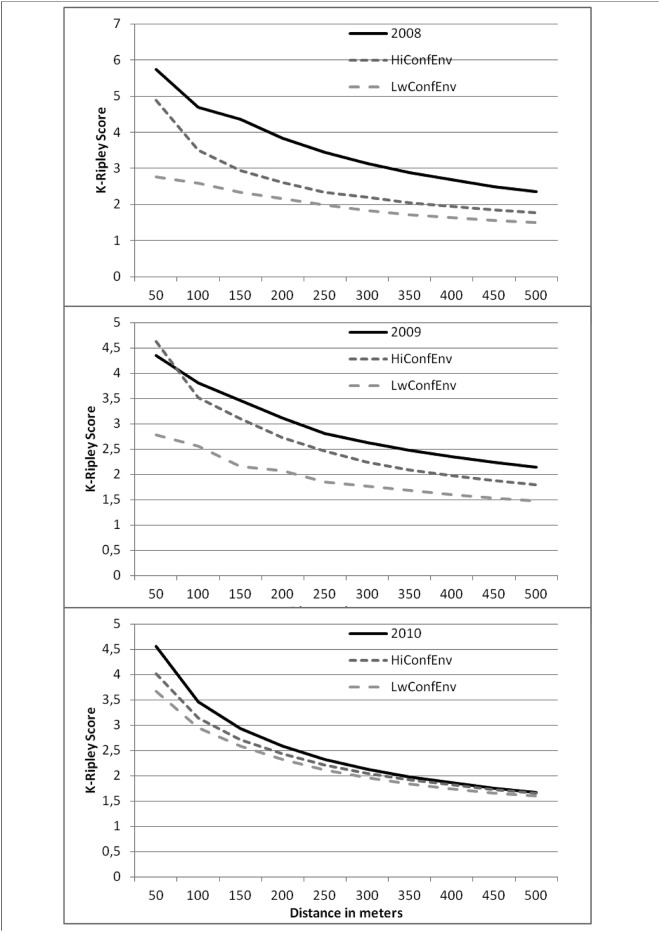
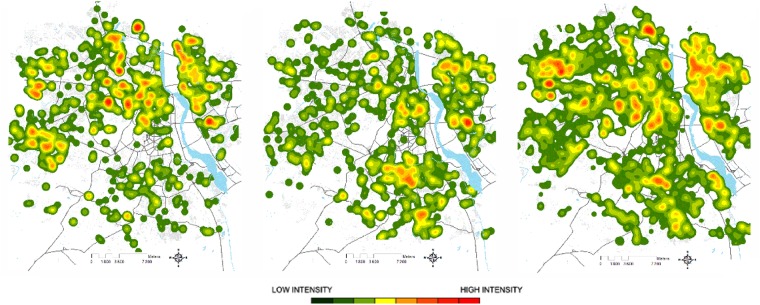
Methodology/principal findings: This Project has been approved by the ethical committee of Institut Pasteur. Data has been anonymized and de-identified prior to geolocalisation and analysis. A GIS was developed for Delhi, enabling typological characterization of the urban environment. Dengue cases identified in the Delhi surveillance system from 2008 to 2010 were collated, localised and embedded within this GIS. The spatio-temporal distribution of dengue cases and extent of clustering were analyzed. Increasing distance from the forest in Delhi reduced the risk of occurrence of a dengue case. Proximity to a hospital did not increase risk of a notified dengue case. Overall, there was high heterogeneity in incidence rate within areas with the same socio-economical profiles and substantial inter-annual variability. Dengue affected the poorest areas with high density of humans, but rich areas were also found to be infected, potentially because of their central location with respect to the daily mobility network of Delhi. Dengue cases were highly clustered in space and there was a strong relationship between the time of introduction of the virus and subsequent cluster size. At a larger scale, earlier introduction predicted the total number of cases.
Conclusions/significance: DENV epidemiology within Delhi has a forest fire signature. The stochastic nature of this invasion process likely smothers any detectable socio-economic risk factors. However, the significant finding that the size of the dengue case cluster depends on the timing of its emergence emphasizes the need for early case detection and implementation of effective mosquito control. A better understanding of the role of population mobility in contributing to dengue risk could also help focus control on areas at particular risk of dengue virus importation.
Conflict of interest statement
Figures
References
-
- Kautner I, Robinson M J, Kuhnle U (1997) Dengue virus infection: Epidemiology, pathogenesis, clinical presentation, diagnosis, and prevention. J Pediatr, 131(4):516–524. - PubMed
-
- Barnes WJ, Rosen L. Fatal (1974) Hemorrhagic disease and shock associated with primary dengue infection on a Pacific island. Am J Trop Med Hyg 23: 495–506. - PubMed
-
- Halstead SB, Udomsakdi S, Singharaj P, Nisalak A. (1969) Dengue and chikungunya virus infection in man in Thailand, 1962–1964. Clinical, epidemiologic, and virologic observations on disease in non-indigenous white persons. Am J Trop Med Hyg 18: 984–96. - PubMed
-
- Gubler D, Kuno G. Dengue and Dengue Hemorrhagic Fever. Wallingford, UK: CAB International; (1997), p 496.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
