

Evaluation of conventional laparoscopic versus robot-assisted laparoscopic redo hiatal hernia and antireflux surgery: a cohort study
- PMID: 26809755
- PMCID: PMC4766202
- DOI: 10.1007/s11701-016-0558-z
Evaluation of conventional laparoscopic versus robot-assisted laparoscopic redo hiatal hernia and antireflux surgery: a cohort study
Abstract
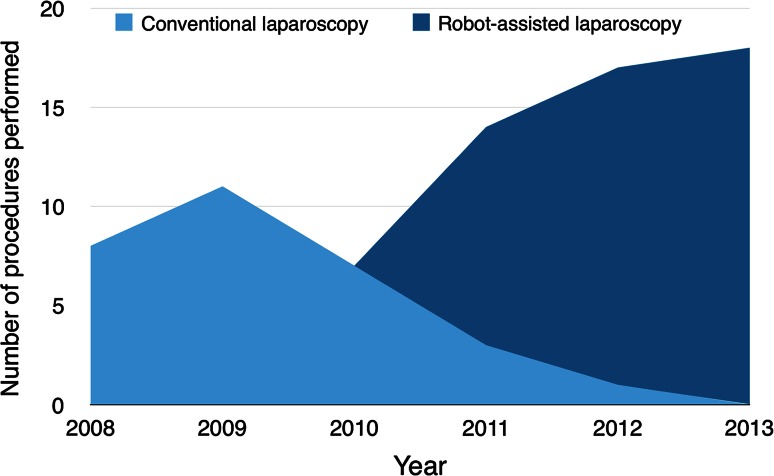
Surgery for refractory gastroesophageal reflux disease (GERD) and hiatal hernia leads to recurrence or persisting dysphagia in a minority of patients. Redo antireflux surgery in GERD and hiatal hernia is known for higher morbidity and mortality. This study aims to evaluate conventional versus robot-assisted laparoscopic redo antireflux surgery, with the objective to detect possible advantages for the robot-assisted approach. A single institute cohort of 75 patients who underwent either conventional laparoscopic or robot-assisted laparoscopic redo surgery for recurrent GERD or severe dysphagia between 2008 and 2013 were included in the study. Baseline characteristics, symptoms, medical history, procedural data, hospital stay, complications and outcome were prospectively gathered. The main indications for redo surgery were dysphagia, pyrosis or a combination of both in combination with a proven anatomic abnormality. The mean time to redo surgery was 1.9 and 2.0 years after primary surgery for the conventional and robot-assisted groups, respectively. The number of conversions was lower in the robot-assisted group compared to conventional laparoscopy (1/45 vs. 5/30, p = 0.035) despite a higher proportion of patients with previous surgery by laparotomy (9/45 vs. 1/30, p = 0.038). Median hospital stay was reduced by 1 day (3 vs. 4, p = 0.042). There were no differences in mortality, complications or outcome. Robotic support, when available, can be regarded beneficial in redo surgery for GERD and hiatal hernia. Results of this observational study suggest technical feasibility for minimal-invasive robot-assisted redo surgery after open primary antireflux surgery, a reduced number of conversions and shorter hospital stay.
Keywords: Da Vinci; Fundoplication; Gastroesophageal reflux; Redo surgery; Robotic surgical procedures.
Figures
References
-
- Pizza F, Rossetti G, Limongelli P, Del Genio G, Maffettone V, Napolitano V, Brusciano L, Russo G, Tolone S, Di Martino M, Del Genio A. Influence of age on outcome of total laparoscopic fundoplication for gastroesophageal reflux disease. World J Gastroenterol. 2007;13:740–747. doi: 10.3748/wjg.v13.i5.740. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
