

Helicopter-based emergency medical services for a sparsely populated region: A study of 42,500 dispatches
- PMID: 26810562
- PMCID: PMC5064740
- DOI: 10.1111/aas.12673
Helicopter-based emergency medical services for a sparsely populated region: A study of 42,500 dispatches
Abstract
Background: The Helicopter Emergency Medical Service (HEMS) in Norway is operated day and night, despite challenging geography and weather. In Western Norway, three ambulance helicopters, with a rapid response car as an alternative, cover close to 1 million inhabitants in an area of 45,000 km(2) . Our objective was to assess patterns of emergency medical problems and treatments in HEMS in a geographically large, but sparsely populated region.
Methods: Data from all HEMS dispatches during 2004-2013 were assessed retrospectively. Information was analyzed with respect to patient treatment and characteristics, in addition to variations in services use during the day, week, and seasons.
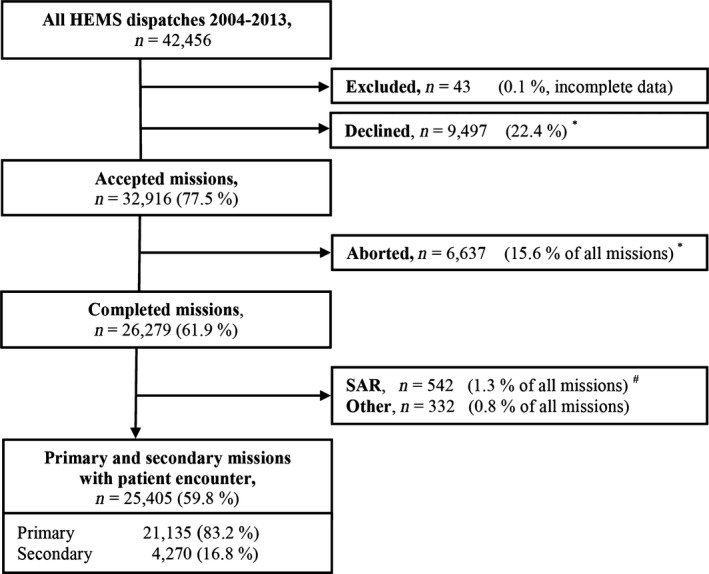
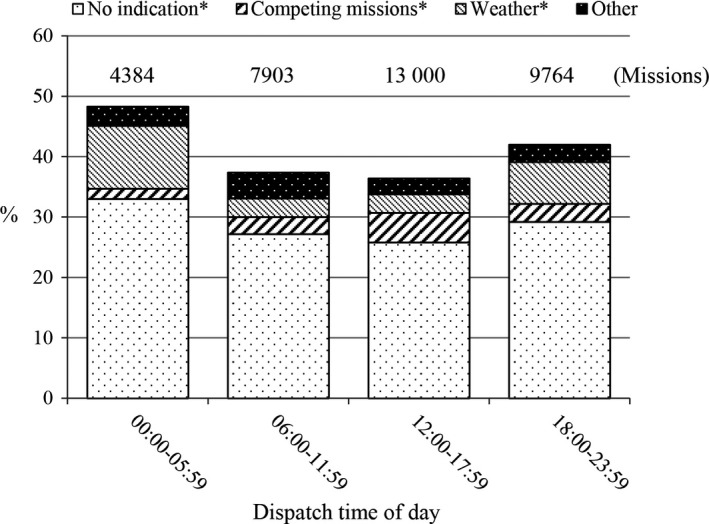
Results: A total of 42,456 dispatches were analyzed. One third of the patients encountered were severely ill or injured, and two thirds of these received advanced treatment. Median activation time and on-scene time in primary helicopter missions were 5 and 11 min, respectively. Most patients (95%) were reached within 45 min by helicopter or rapid response car. Patterns of use did not change. More than one third of all dispatches were declined or aborted, mostly due to no longer medical indication, bad weather conditions, or competing missions.
Conclusion: One third of the patients encountered were severely ill or injured, and more than two thirds of these received advanced treatment. HEMS use did not change over the 10-year period, however HEMS use peaked during daytime, weekends, and the summer. More than one third of all dispatches were declined or aborted.
© 2015 The Authors. Acta Anaesthesiologica Scandinavica published by John Wiley & Sons Ltd on behalf of Acta Anaesthesiologica Scandinavica Foundation.
Figures

Similar articles
-
Characteristics of patients treated by the Danish Helicopter Emergency Medical Service from 2014-2018: a nationwide population-based study.Scand J Trauma Resusc Emerg Med. 2019 Nov 7;27(1):102. doi: 10.1186/s13049-019-0672-9. Scand J Trauma Resusc Emerg Med. 2019. PMID: 31699120 Free PMC article.
-
A Physician-Based Helicopter Emergency Medical Services Was Associated With an Additional 2.5 Lives Saved per 100 Dispatches of Severely Injured Pediatric Patients.Air Med J. 2019 Jul-Aug;38(4):289-293. doi: 10.1016/j.amj.2019.04.003. Epub 2019 May 23. Air Med J. 2019. PMID: 31248540
-
Helicopter emergency medical services in Iceland between 2018 and 2022-A retrospective study.Acta Anaesthesiol Scand. 2024 Nov;68(10):1494-1503. doi: 10.1111/aas.14509. Epub 2024 Aug 7. Acta Anaesthesiol Scand. 2024. PMID: 39113192
-
A 26-year comparative review of United Kingdom helicopter emergency medical services crashes and serious incidents.J Trauma Acute Care Surg. 2014 Apr;76(4):1055-60. doi: 10.1097/TA.0000000000000170. J Trauma Acute Care Surg. 2014. PMID: 24662871 Review.
-
[Air rescue: current significance and practical issues].Anaesthesist. 2014 Dec;63(12):971-80; quiz 981-2. doi: 10.1007/s00101-014-2356-1. Anaesthesist. 2014. PMID: 25430664 Review. German.
Cited by
-
Nine golden codes: improving the accuracy of Helicopter Emergency Medical Services (HEMS) dispatch-a retrospective, multi-organisational study in the East of England.Scand J Trauma Resusc Emerg Med. 2023 Jun 12;31(1):27. doi: 10.1186/s13049-023-01094-w. Scand J Trauma Resusc Emerg Med. 2023. PMID: 37308937 Free PMC article.
-
Impact of icing weather conditions on the patients in helicopter emergency medical service: a prospective study from Northern Finland.Scand J Trauma Resusc Emerg Med. 2019 Feb 12;27(1):13. doi: 10.1186/s13049-019-0592-8. Scand J Trauma Resusc Emerg Med. 2019. PMID: 30755241 Free PMC article.
-
Mortality rates in Norwegian HEMS-a retrospective analysis from Central Norway.Scand J Trauma Resusc Emerg Med. 2024 Apr 16;32(1):29. doi: 10.1186/s13049-024-01202-4. Scand J Trauma Resusc Emerg Med. 2024. PMID: 38627817 Free PMC article.
-
Characteristics of helicopter emergency medical services (HEMS) dispatch cancellations during a six-year period in a Dutch HEMS region.BMC Emerg Med. 2021 Apr 16;21(1):50. doi: 10.1186/s12873-021-00439-x. BMC Emerg Med. 2021. PMID: 33863280 Free PMC article.
-
The Danish helicopter emergency medical service database: high quality data with great potential.Scand J Trauma Resusc Emerg Med. 2019 Apr 5;27(1):38. doi: 10.1186/s13049-019-0615-5. Scand J Trauma Resusc Emerg Med. 2019. PMID: 30953564 Free PMC article.
References
-
- Øgar P. NOU 1998:8 Air ambulance service in Norway (Document in Norwegian). SHD 1998: 161.
-
- Kruger AJ, Skogvoll E, Castren M, Kurola J, Lossius HM. Scandinavian pre‐hospital physician‐manned Emergency Medical Services – same concept across borders? Resuscitation 2010; 81: 427–33. - PubMed
-
- Kaufmann M, Moser B, Lederer W. Changes in injury patterns and severity in a helicopter air‐rescue system over a 6‐year period. Wilderness Environ Med 2006; 17: 8–14. - PubMed
-
- Leaman AM, Nutbeam T. Trauma systems and medical helicopters in the UK. Injury 2011; 42: 12–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
