

Novel Bloodless Potassium Determination Using a Signal-Processed Single-Lead ECG
- PMID: 26811164
- PMCID: PMC4859394
- DOI: 10.1161/JAHA.115.002746
Novel Bloodless Potassium Determination Using a Signal-Processed Single-Lead ECG
Abstract
Background: Hyper- and hypokalemia are clinically silent, common in patients with renal or cardiac disease, and are life threatening. A noninvasive, unobtrusive, blood-free method for tracking potassium would be an important clinical advance.
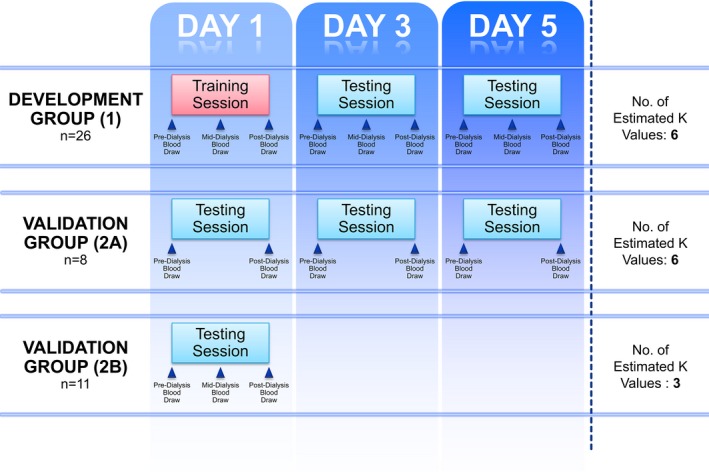
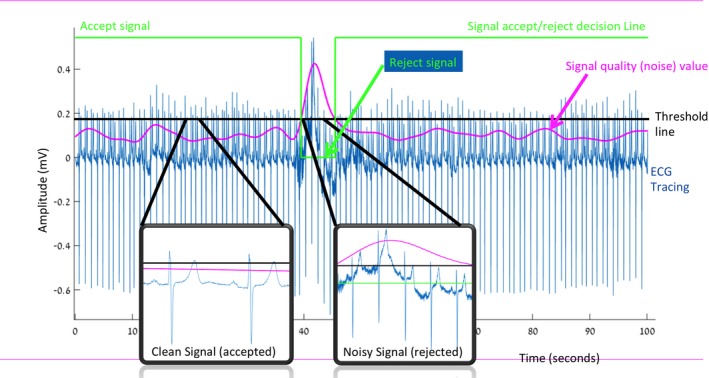
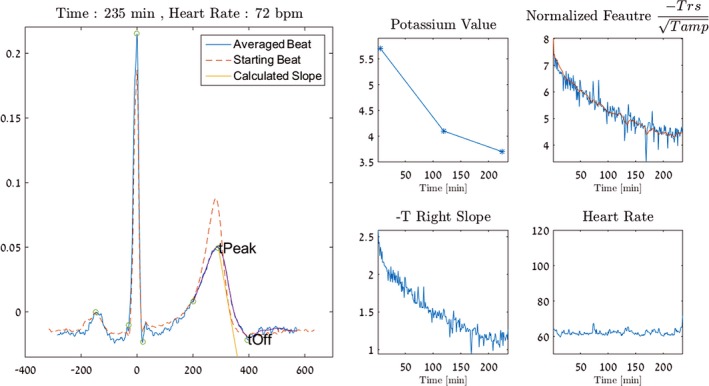
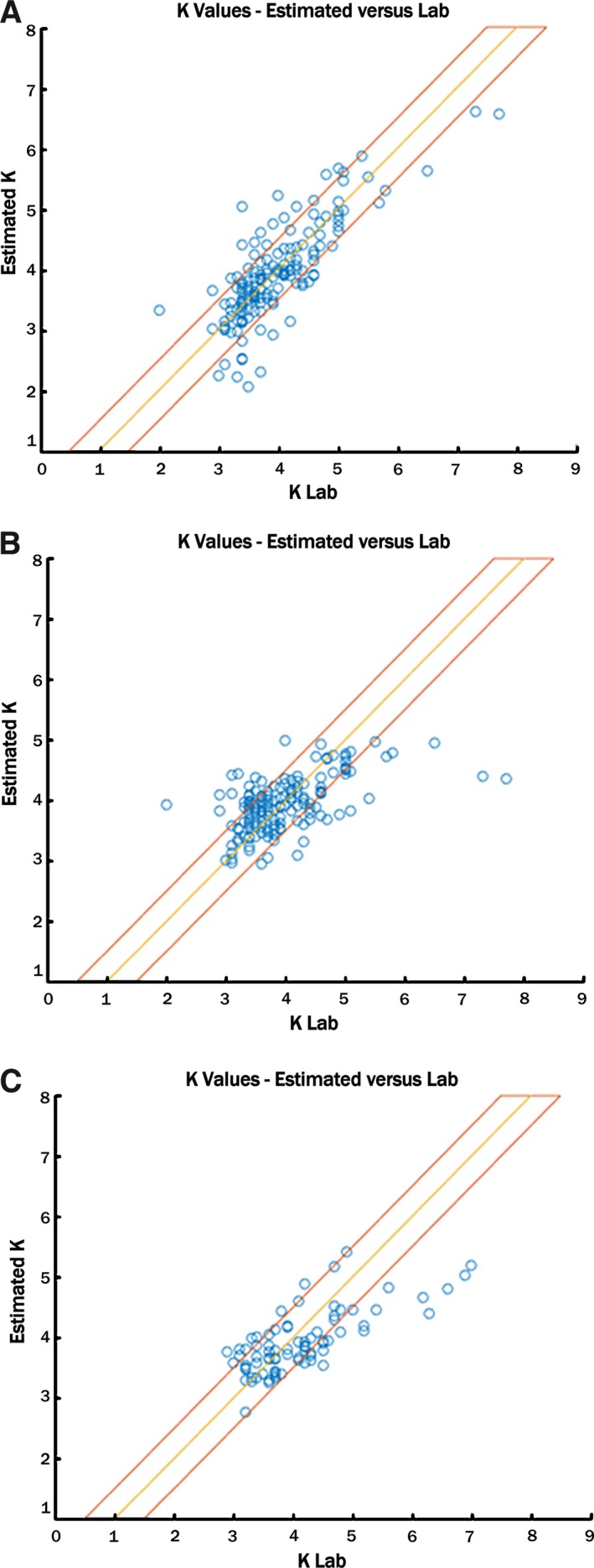
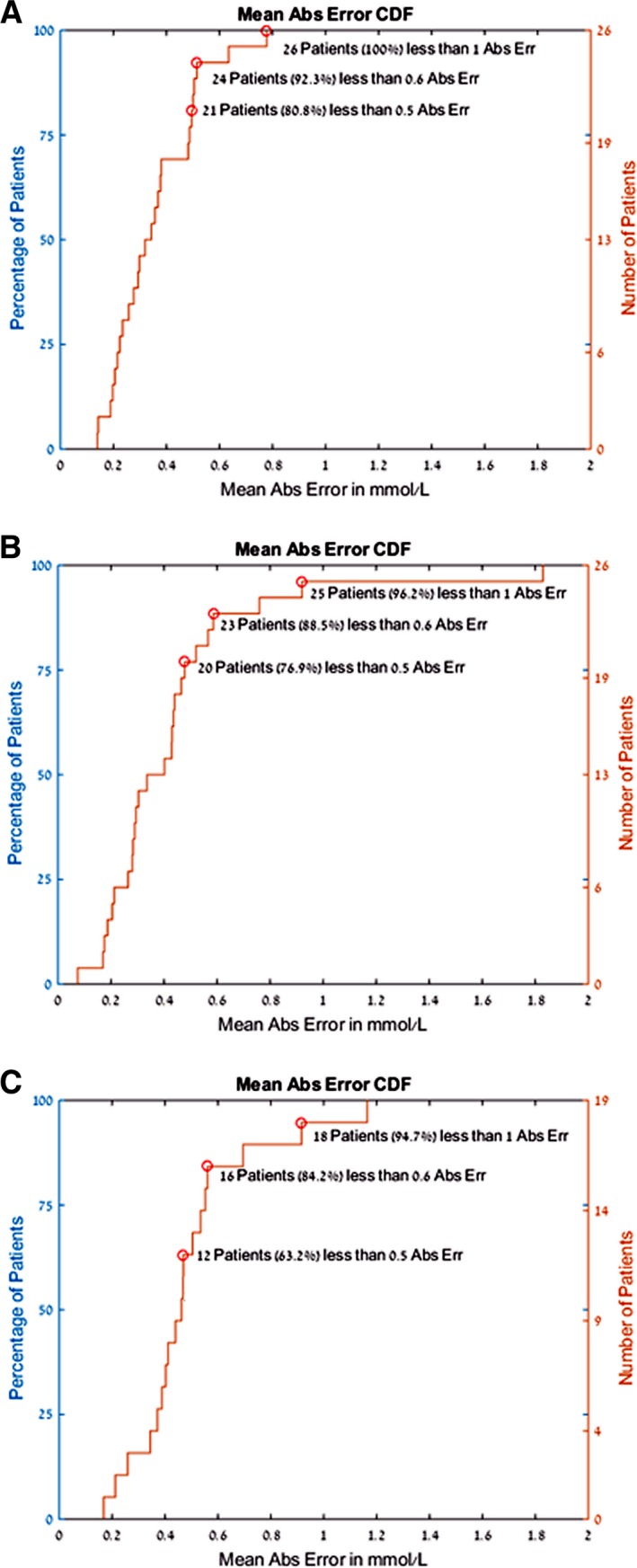
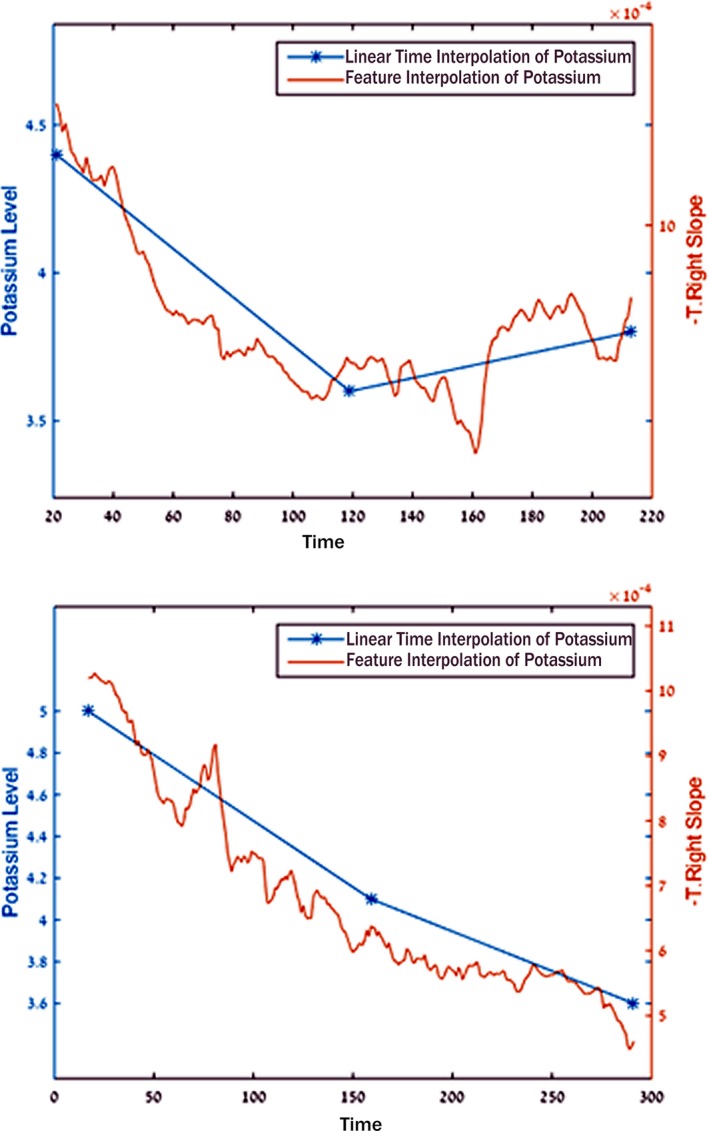
Methods and results: Two groups of hemodialysis patients (development group, n=26; validation group, n=19) underwent high-resolution digital ECG recordings and had 2 to 3 blood tests during dialysis. Using advanced signal processing, we developed a personalized regression model for each patient to noninvasively calculate potassium values during the second and third dialysis sessions using only the processed single-channel ECG. In addition, by analyzing the entire development group's first-visit data, we created a global model for all patients that was validated against subsequent sessions in the development group and in a separate validation group. This global model sought to predict potassium, based on the T wave characteristics, with no blood tests required. For the personalized model, we successfully calculated potassium values with an absolute error of 0.36±0.34 mmol/L (or 10% of the measured blood potassium). For the global model, potassium prediction was also accurate, with an absolute error of 0.44±0.47 mmol/L for the training group (or 11% of the measured blood potassium) and 0.5±0.42 for the validation set (or 12% of the measured blood potassium).
Conclusions: The signal-processed ECG derived from a single lead can be used to calculate potassium values with clinically meaningful resolution using a strategy that requires no blood tests. This enables a cost-effective, noninvasive, unobtrusive strategy for potassium assessment that can be used during remote monitoring.
Keywords: electrophysiology; potassium; waves.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Goyal A, Spertus JA, Gosch K, Venkitachalam L, Jones PG, Van den Berghe G, Kosiborod M. Serum potassium levels and mortality in acute myocardial infarction. JAMA. 2012;307:157–164. - PubMed
-
- Gennari FJ. Hypokalemia. N Engl J Med. 1998;339:451–458. - PubMed
-
- Kovesdy CP. Management of hyperkalaemia in chronic kidney disease. Nat Rev Nephrol. 2014;10:653–662. - PubMed
-
- Weiner ID, Wingo CS. Hyperkalemia: a potential silent killer. J Am Soc Nephrol. 1998;9:1535–1543. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
