

Hearing Loss in Patients Who Received Cranial Radiation Therapy for Childhood Cancer
- PMID: 26811531
- PMCID: PMC4933129
- DOI: 10.1200/JCO.2015.63.6738
Hearing Loss in Patients Who Received Cranial Radiation Therapy for Childhood Cancer
Abstract
Purpose: Patients treated with cranial radiation therapy (RT) are at risk for sensorineural hearing loss (SNHL). Although SNHL is often characterized as a delayed consequence of anticancer therapy, longitudinal reports of SNHL in childhood cancer survivors treated with contemporary RT are limited. We report the incidence, onset, severity, and long-term trajectory of SNHL among children receiving RT. Potential risk factors for SNHL were also identified.
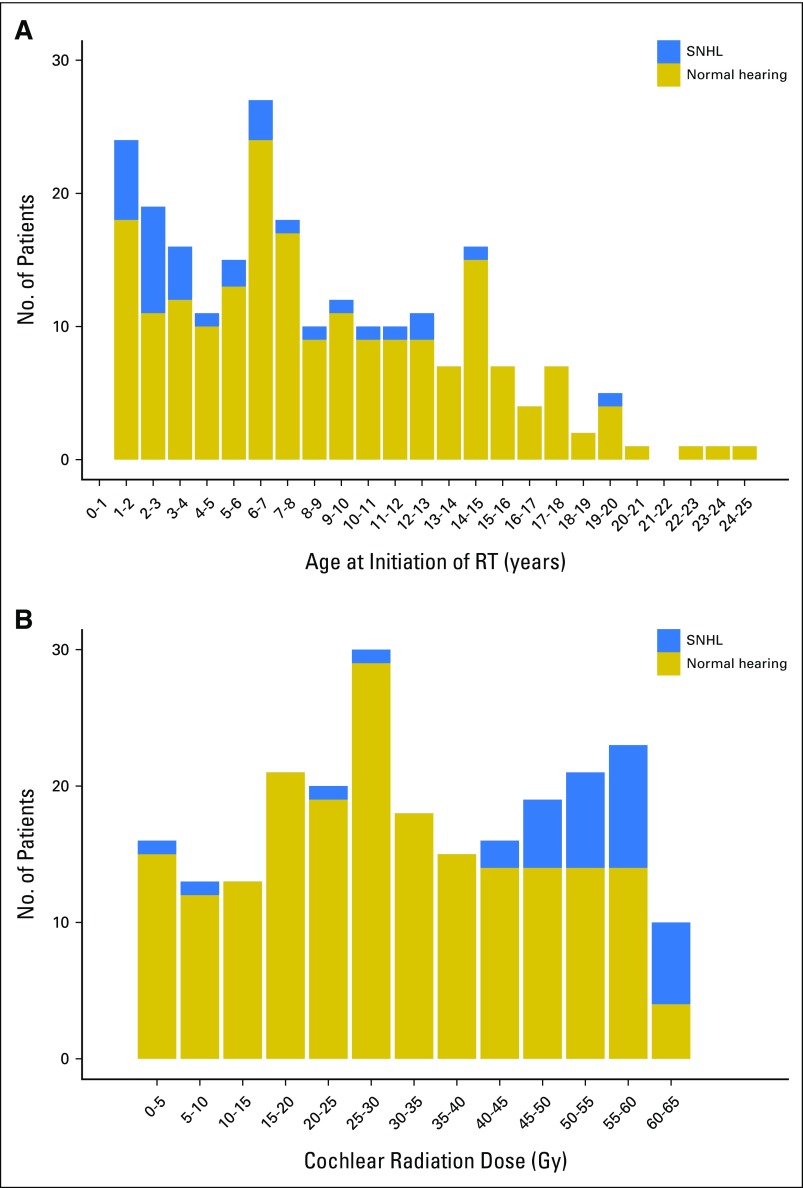
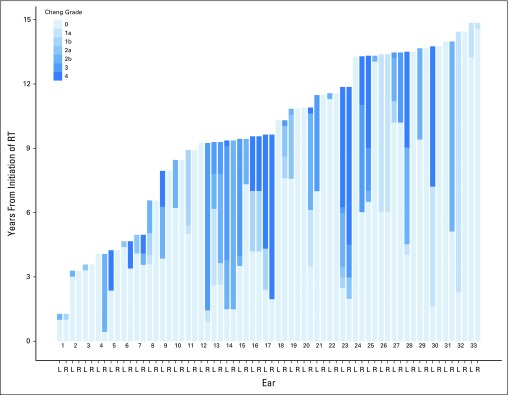
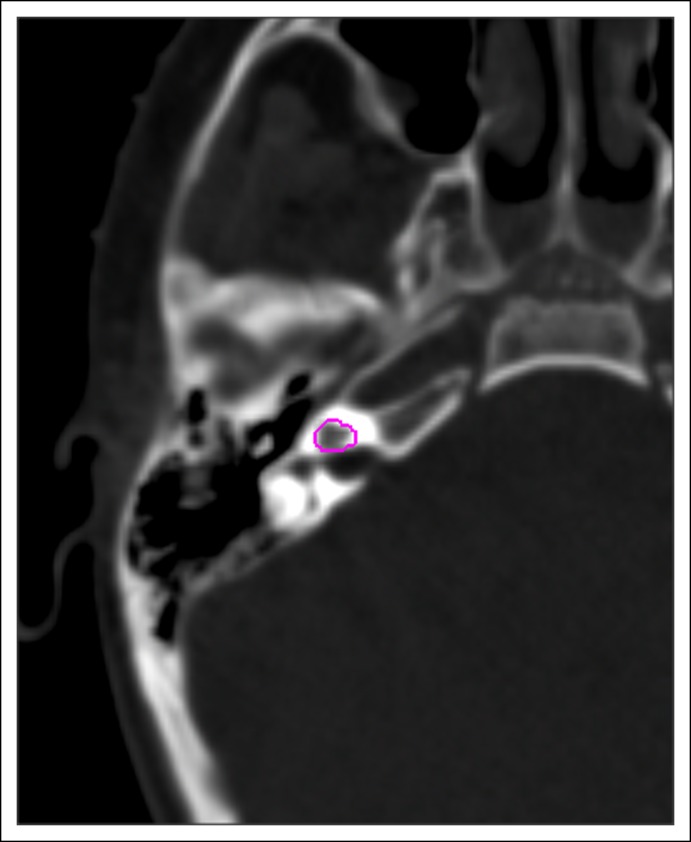
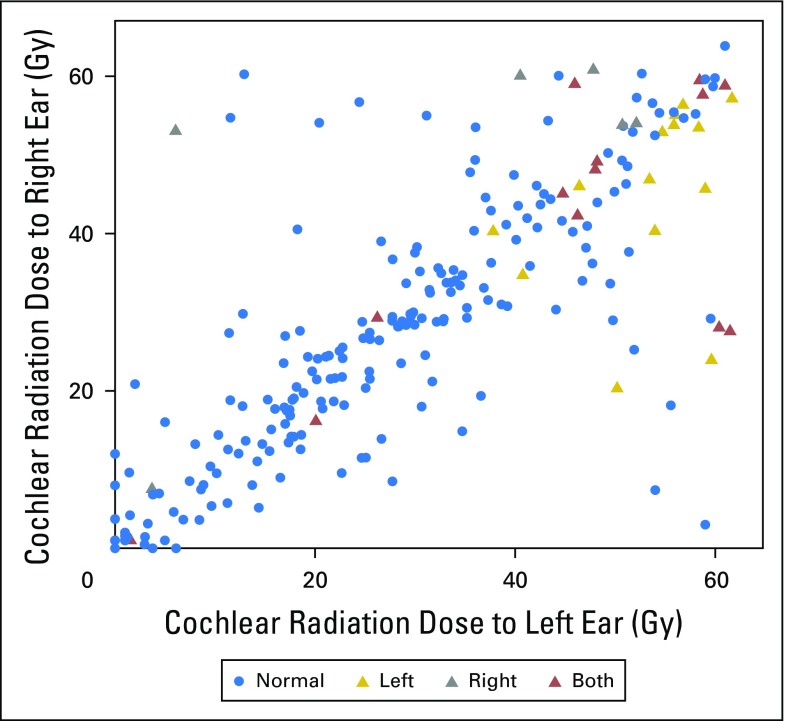
Patients and methods: Serial audiologic testing was conducted on 235 pediatric patients who were treated with conformal or intensity-modulated RT as part of an institutional phase II trial for localized primary brain tumors, including craniopharyngioma, ependymoma, and juvenile pilocytic astrocytoma. All but one patient had measurable cochlear radiation dose (CRD) greater than 0 Gy. The median follow-up from RT initiation to latest audiogram was 9 years with a median of 11 post-RT audiograms per patient. Audiograms were classified by the Chang Ototoxicity Grading Scale. Progression was defined by an increase in Chang grade from SNHL onset to the most recent evaluation.
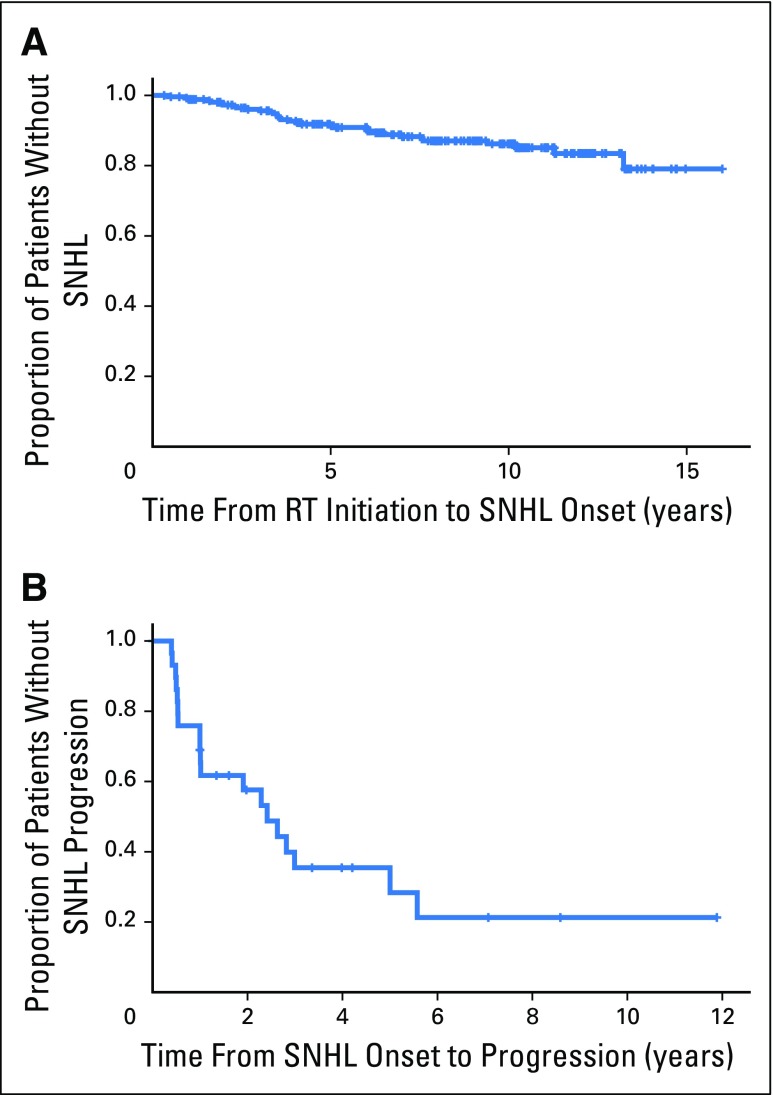
Results: At last evaluation, SNHL was prevalent in 14% of patients: 2.1% had mild and 11.9% had significant SNHL requiring hearing aids. Median time from RT to SNHL onset was 3.6 years (range, 0.4 to 13.2 years). Among 29 patients with follow-up evaluations after SNHL onset, 65.5% experienced continued decline in hearing sensitivity in either ear and 34.5% had no change. Younger age at RT initiation (hazard ratio [HR], 2.32; 95% CI, 1.21 to 4.46), higher CRD (HR, 1.07; 95% CI, 1.03 to 1.11), and cerebrospinal fluid shunting (HR, 2.02; 95% CI, 1.07 to 3.78) were associated with SNHL.
Conclusion: SNHL is a late effect of RT that likely worsens over time. Long-term audiologic follow-up for a minimum of 10 years post-RT is recommended.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at
Figures
References
-
- Ho WK, Wei WI, Kwong DL, et al. Long-term sensorineural hearing deficit following radiotherapy in patients suffering from nasopharyngeal carcinoma: A prospective study. Head Neck. 1999;21:547–553. - PubMed
-
- Merchant TE, Gould CJ, Xiong X, et al. Early neuro-otologic effects of three-dimensional irradiation in children with primary brain tumors. Int J Radiat Oncol Biol Phys. 2004;58:1194–1207. - PubMed
-
- Hua C, Bass JK, Khan R, et al. Hearing loss after radiotherapy for pediatric brain tumors: Effect of cochlear dose. Int J Radiat Oncol Biol Phys. 2008;72:892–899. - PubMed
-
- Low WK, Toh ST, Wee J, et al. Sensorineural hearing loss after radiotherapy and chemoradiotherapy: A single, blinded, randomized study. J Clin Oncol. 2006;24:1904–1909. - PubMed
-
- Bhandare N, Antonelli PJ, Morris CG, et al. Ototoxicity after radiotherapy for head and neck tumors. Int J Radiat Oncol Biol Phys. 2007;67:469–479. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
