

Impact of immediate versus delayed tracheal extubation on length of ICU stay of cardiac surgical patients, a randomized trial
- PMID: 26811837
- PMCID: PMC4712034
Impact of immediate versus delayed tracheal extubation on length of ICU stay of cardiac surgical patients, a randomized trial
Abstract
Introduction: Ultra-fast track anaesthesia aims at immediate extubation of cardiac surgical patients at the end of the operation. This study compares the effect of ultrafast track anesthesia versus continued postoperative mechanical ventilation on the intensive care unit length of stay.
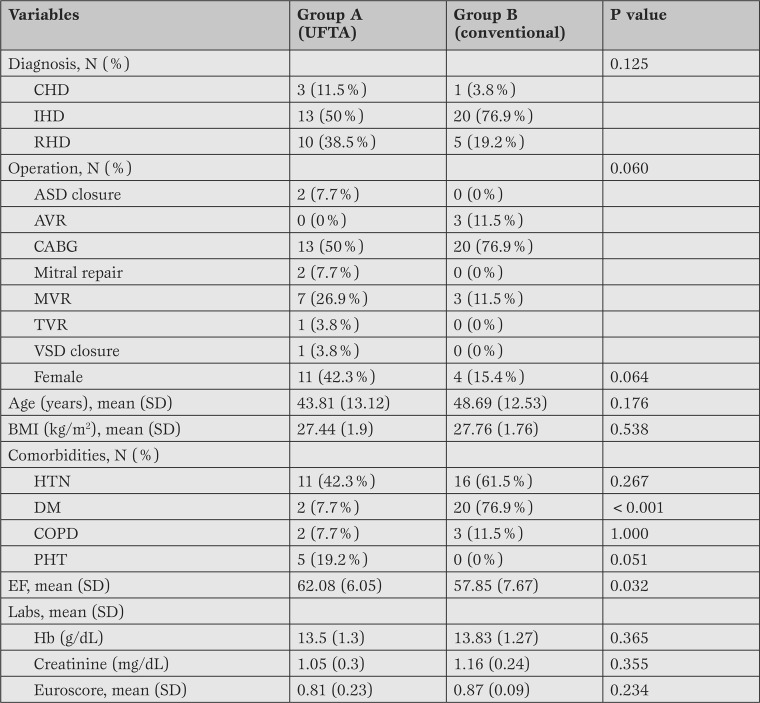
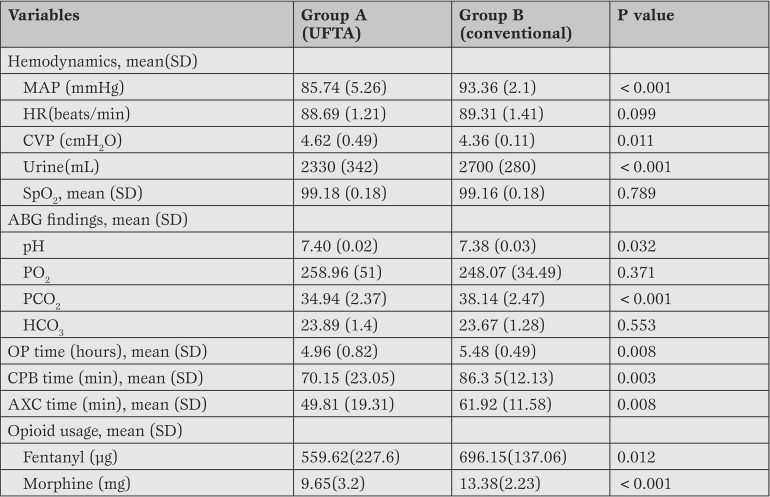
Methods: Fifty-two elective adult patients were randomly allocated into ultrafast track anaesthesia and conventional groups by computer-generated random numbers. Redo operations, pre-operative intubation, uncontrolled diabetes, shock/left ventricular ejection fraction < 45%, pulmonary artery systolic pressure >55mmHg, creatinine clearance -1, haemodynamic instability, or those with concerns of postoperative bleeding were excluded. Pre- and intra-operative management was similar and Logistic EuroSCORE II was calculated for all. Intra-operatively, haemodynamic parameters, urine output, oxygen saturation, arterial blood gas analysis, 5-lead electrocardiogram, operative bypass- and cross-clamp time, and opioid consumption were collected. Postoperatively, patients were compared during their intensive care unit stay. Data were analysed by χ²/Fischer exact, unpaired student's t-test, univariate two-group repeated measures with post hoc Dunnett's test, and Mann-Whitney U tests as appropriate. p < 0.05 was considered significant.
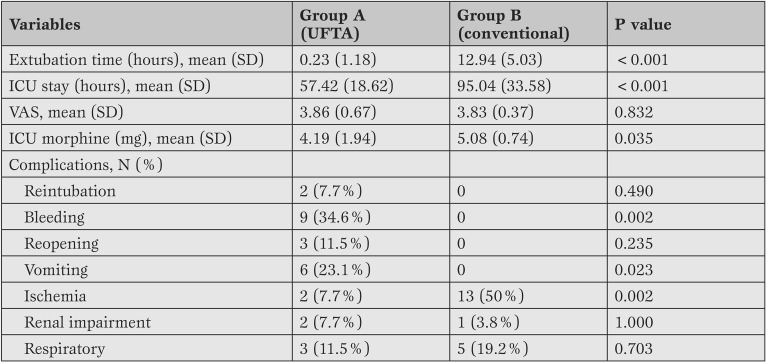
Results: Patients were comparable regarding their peri-operative characteristics and EuroSCORE. The intensive care unit stay was shorter in the ultrafast track anaesthesia group [57.4 (18.6) vs. 95 (33.6) h. p < 0.001], without increasing postoperative renal, respiratory complications rate or reopening rate.
Conclusions: In this single center study, ultrafast track anaesthesia decreased intensive care unit stay without increasing the rate of post-operative complications.
Keywords: ICU stay; cardiac anaesthesia; ultra fast track anaesthesia.
Conflict of interest statement
Figures
References
-
- Montes F R, Sanchez S I, Giraldo J C, Rincón J D, RincÓn I E, Vanegas M V. et al. The lack of benefit of tracheal extubation in the operating room after coronary artery bypass surgery. Anesth Analg. 2000;91:776–780. - PubMed
-
- Berry P, Thomas S, Mahon S, Jackson M, Fox M, Fabri B. et al. Myocardial ischaemia after coronary artery bypass grafting: early vs late extubation. Br J Anaesth. 1998;80:20–20. - PubMed
-
- Bainbridge D, Cheng D. Initial Perioperative Care of the Cardiac Surgical Patient. Semin Cardiothorac Vasc Anesth. 2002;6:229–236.
-
- Cheng DC, Karski J, Peniston C, Raveendran G, Asokumar B, Carroll J. et al. Early tracheal extubation after coronary artery bypass graft surgery reduces costs and improves resource use. A prospective, randomized, controlled trial. Anesthesiology. 1996;85:1300–1310. - PubMed
-
- Lazar HL, Fitzgerald CA, Ahmad T, Bao Y, Colton T, Shapira OM. et al. Early discharge after coronary artery bypass graft surgery: are patients really going home earlier? J Thorac Cardiovasc Surg. 2001;121:943–950. - PubMed
LinkOut - more resources
Full Text Sources
Medical