

An Alzheimer's Disease-Derived Biomarker Signature Identifies Parkinson's Disease Patients with Dementia
- PMID: 26812251
- PMCID: PMC4727929
- DOI: 10.1371/journal.pone.0147319
An Alzheimer's Disease-Derived Biomarker Signature Identifies Parkinson's Disease Patients with Dementia
Abstract
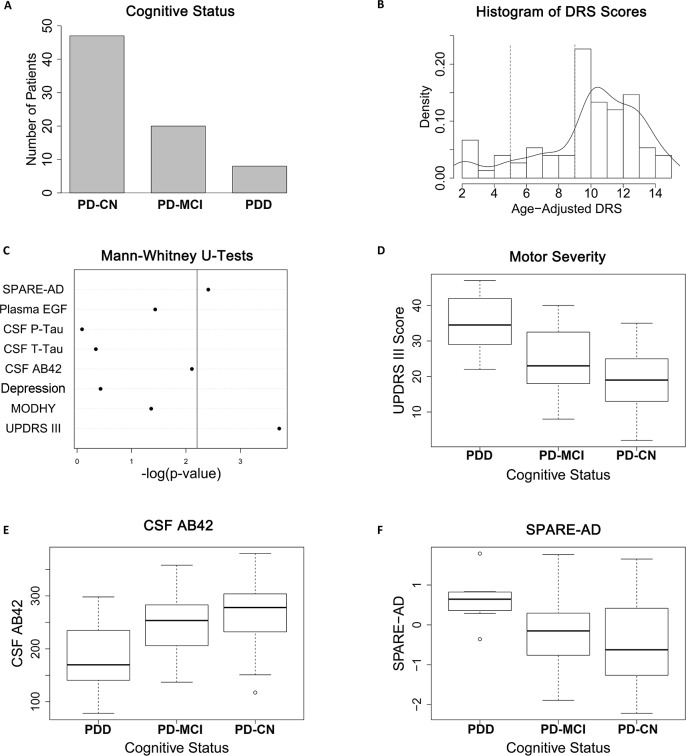
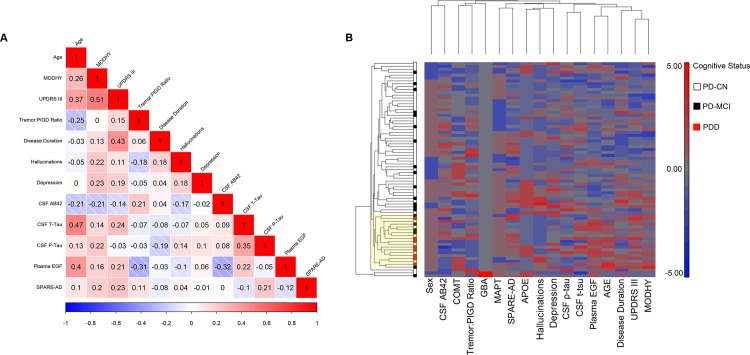
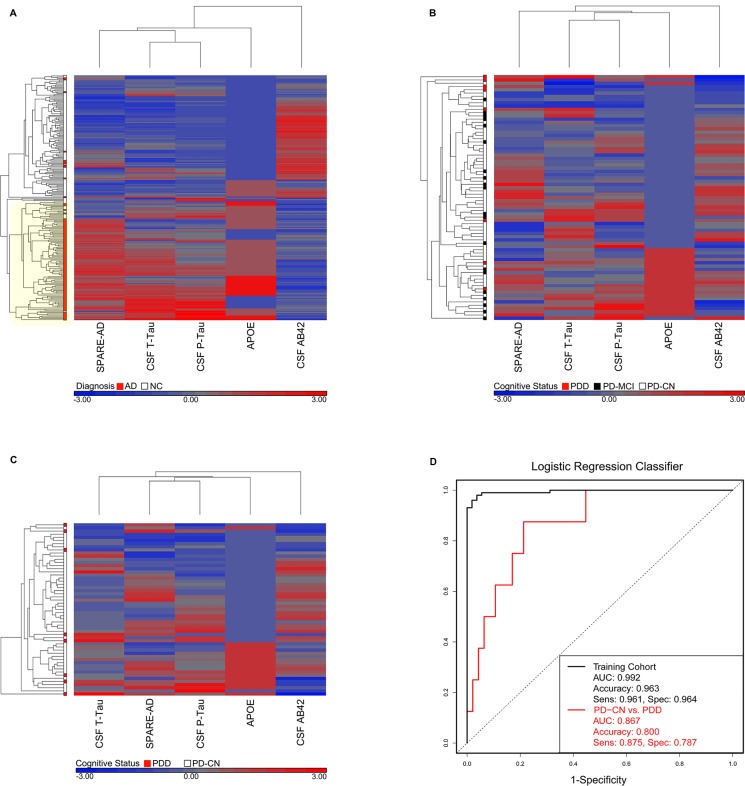
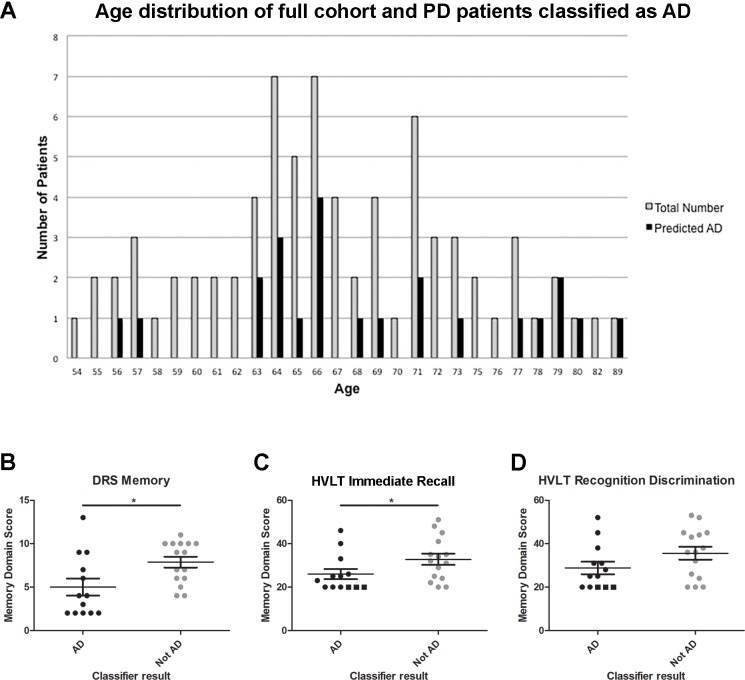
Biomarkers from multiple modalities have been shown to correlate with cognition in Parkinson's disease (PD) and in Alzheimer's disease (AD). However, the relationships of these markers with each other, and the use of multiple markers in concert to predict an outcome of interest, are areas that are much less explored. Our objectives in this study were (1) to evaluate relationships among 17 biomarkers previously reported to associate with cognition in PD or AD and (2) to test performance of a five-biomarker classifier trained to recognize AD in identifying PD with dementia (PDD). To do this, we evaluated a cross-sectional cohort of PD patients (n = 75) across a spectrum of cognitive abilities. All PD participants had 17 baseline biomarkers from clinical, genetic, biochemical, and imaging modalities measured, and correlations among biomarkers were assessed by Spearman's rho and by hierarchical clustering. We found that internal correlation among all 17 candidate biomarkers was modest, showing a maximum pairwise correlation coefficient of 0.51. However, a five-marker subset panel derived from AD (CSF total tau, CSF phosphorylated tau, CSF amyloid beta 42, APOE genotype, and SPARE-AD imaging score) discriminated cognitively normal PD patients vs. PDD patients with 80% accuracy, when employed in a classifier originally trained to recognize AD. Thus, an AD-derived biomarker signature may identify PDD patients with moderately high accuracy, suggesting mechanisms shared with AD in some PDD patients. Based on five measures readily obtained during life, this AD-derived signature may prove useful in identifying PDD patients most likely to respond to AD-based crossover therapies.
Conflict of interest statement
Figures
References
-
- Tanzi RE, Bertram L. Twenty years of the Alzheimer’s disease amyloid hypothesis: a genetic perspective. Cell. 2005;120: 545–555. - PubMed
-
- Fearnley JM, Lees AJ. Ageing and Parkinson's disease: substantia nigra regional selectivity. Brain. 1991;114 (Pt 5): 2283–2301. - PubMed
-
- Williams-Gray CH, Foltynie T, Brayne CE, Robbins TW, Barker RA. Evolution of cognitive dysfunction in an incident Parkinson's disease cohort. Brain. 2007;130: 1787–1798. - PubMed
-
- Hely MA, Reid WG, Adena MA, Halliday GM, Morris JG. The Sydney multicenter study of Parkinson's disease: the inevitability of dementia at 20 years. 2008;23: 837–844. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
