

Change in Adverse Events After Enrollment in the National Surgical Quality Improvement Program: A Systematic Review and Meta-Analysis
- PMID: 26812596
- PMCID: PMC4727780
- DOI: 10.1371/journal.pone.0146254
Change in Adverse Events After Enrollment in the National Surgical Quality Improvement Program: A Systematic Review and Meta-Analysis
Abstract
Background: The American College of Surgeons' National Surgical Quality Improvement Program (NSQIP) is the first nationally validated, risk-adjusted, outcomes-based program to measure and compare the quality of surgical care across North America. Participation in this program may provide an opportunity to reduce the incidence of adverse events related to surgery.
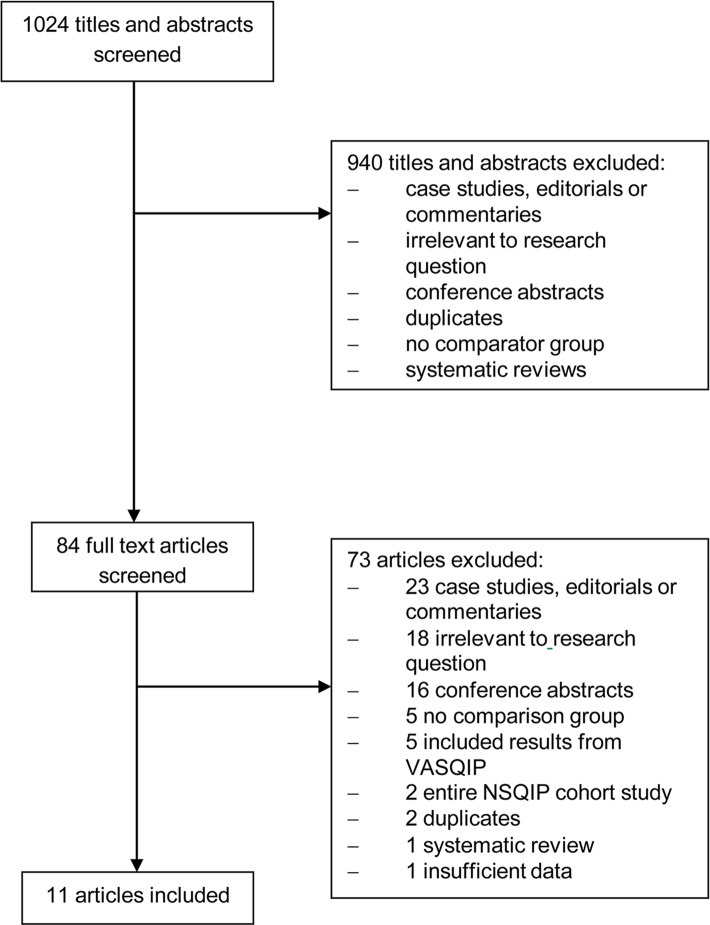
Study design: A systematic review of the literature was performed. MedLine, EMBASE and PubMed were searched for studies relevant to NSQIP. Patient characteristics, intervention, and primary outcome measures were abstracted. The intervention was participation in NSQIP and monitoring of Individual Site Summary Reports with or without implementation of a quality improvement program. The outcomes of interest were change in peri-operative adverse events and mortality represented by pooled risk ratios (pRR) and 95% confidence intervals (CI).
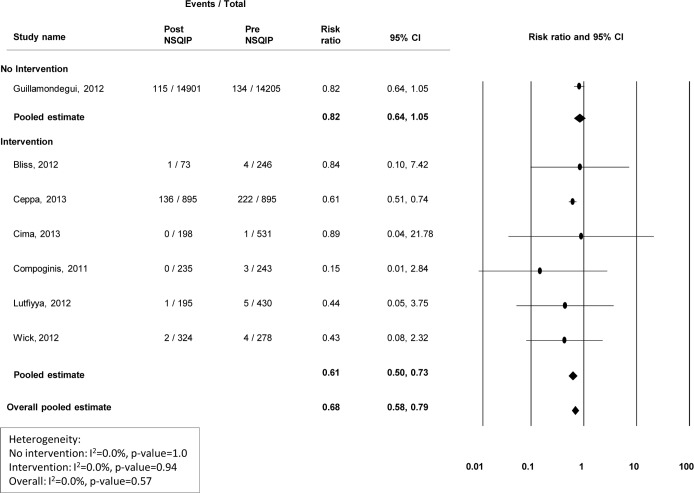
Results: Eleven articles reporting on 35 health care institutions were included. Nine (82%) of the eleven studies implemented a quality improvement program. Minimal improvements in superficial (pRR 0.81; 95% CI 0.72-0.91), deep (pRR 0.82; 95% CI0.64-1.05) and organ space (pRR 1.15; 95% CI 0.96-1.37) infections were observed at centers that did not institute a quality improvement program. However, centers that reported formal interventions for the prevention and treatment of infections observed substantial improvements (superficial pRR 0.55, 95% CI 0.39-0.77; deep pRR 0.61, 95% CI 0.50-0.75, and organ space pRR 0.60, 95% CI 0.50-0.71). Studies evaluating other adverse events noted decreased incidence following NSQIP participation and implementation of a formal quality improvement program.
Conclusions: These data suggest that NSQIP is effective in reducing surgical morbidity. Improvement in surgical quality appears to be more marked at centers that implemented a formal quality improvement program directed at the reduction of specific morbidities.
Conflict of interest statement
Figures





References
-
- Cohen ME, Ko CY, Bilimoria KY, Zhou L, Huffman K, Wang X, et al. Optimizing ACS NSQIP modeling for evaluation of surgical quality and risk: patient risk adjustment, procedure mix adjustment, shrinkage adjustment, and surgical focus. J Am Coll Surg 2013;217(2):336–346.e331. 10.1016/j.jamcollsurg.2013.02.027 - DOI - PubMed
-
- Shiloach M, Frencher SK Jr, Steeger JE, Rowell K, Bartzokis K, Tomeh MG, et al. Toward robust information: data quality and inter-rater reliability in the American College of Surgeons National Surgical Quality Improvement Program. J Am Coll Surg 2010;210(1):6–16. 10.1016/j.jamcollsurg.2009.09.031 - DOI - PubMed
-
- American College of Surgeons National Surgical Quality Improvement Program. User Guide for the Participant Use Data File. Available: http://site.acsnsqip.org/wp-content/uploads/2012/03/ACS-NSQIP-Participan....
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
