

Significant treatment effect of adjunct music therapy to standard treatment on the positive, negative, and mood symptoms of schizophrenic patients: a meta-analysis
- PMID: 26812906
- PMCID: PMC4728768
- DOI: 10.1186/s12888-016-0718-8
Significant treatment effect of adjunct music therapy to standard treatment on the positive, negative, and mood symptoms of schizophrenic patients: a meta-analysis
Erratum in
-
Erratum to: Significant treatment effect of adjunct music therapy to standard treatment on the positive, negative, and mood symptoms of schizophrenic patients: a meta-analysis.BMC Psychiatry. 2016 May 17;16:150. doi: 10.1186/s12888-016-0846-1. BMC Psychiatry. 2016. PMID: 27188423 Free PMC article. No abstract available.
Abstract
Background: Music therapy (MT) has been used as adjunct therapy for schizophrenia for decades. However, its role is still inconclusive. A recent meta-analysis demonstrated that MT for schizophrenic patients only significantly benefits negative symptoms and mood symptoms rather than positive symptoms. In addition, the association between specific characteristics of MT and the treatment effect remains unclear. The aim of this study was to update the published data and to explore the role of music therapy in adjunct treatment in schizophrenia with a thorough meta-analysis.
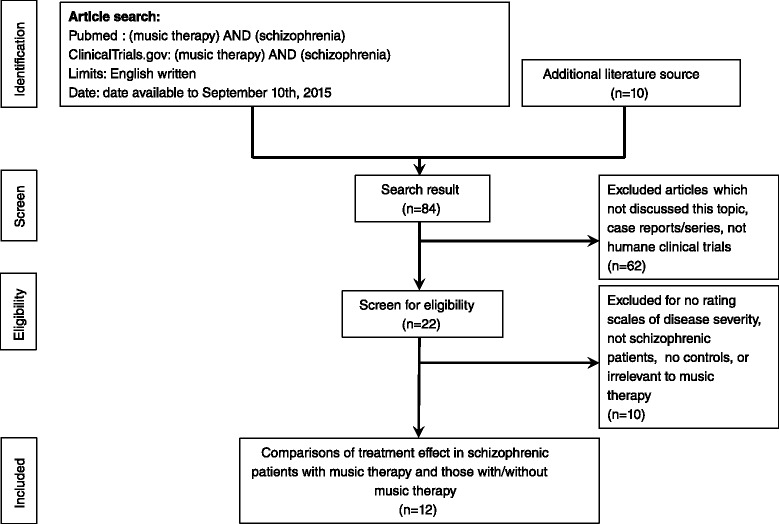
Methods: We compared the treatment effect in schizophrenic patients with standard treatment who did and did not receive adjunct MT through a meta-analysis, and investigated the clinical characteristics of MT through meta-regression.
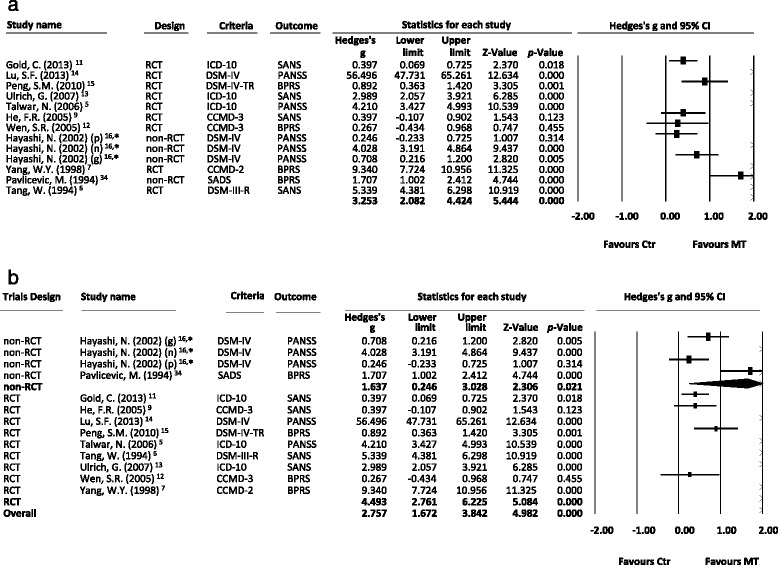
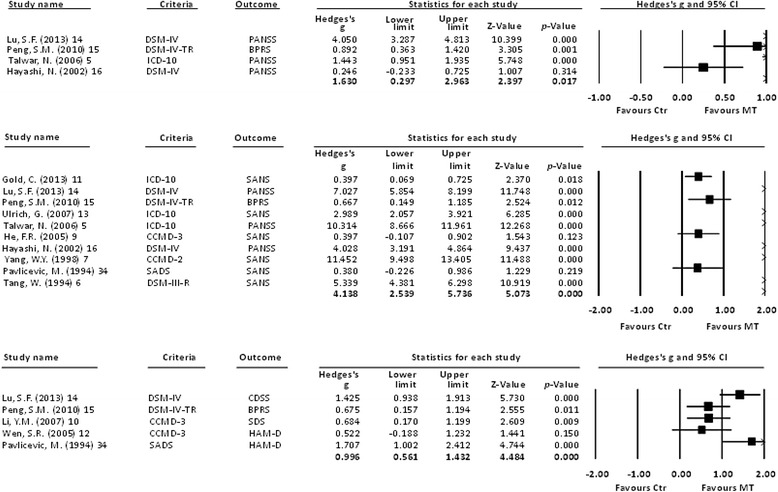
Results: The main finding was that the treatment effect was significantly better in the patients who received adjunct MT than in those who did not, in negative symptoms, mood symptoms, and also positive symptoms (all p < 0.05). This significance did not change after dividing the patients into subgroups of different total duration of MT, amounts of sessions, or frequency of MT. Besides, the treatment effect on the general symptoms was significantly positively associated with the whole duration of illness, indicating that MT would be beneficial for schizophrenic patients with a chronic course.
Conclusions: Our meta-analysis highlights a significantly better treatment effect in schizophrenic patients who received MT than in those who did not, especially in those with a chronic course, regardless of the duration, frequency, or amounts of sessions of MT. These findings provide evidence that clinicians should apply MT for schizophrenic patients to alleviate disease severity.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
