

MoodHacker Mobile Web App With Email for Adults to Self-Manage Mild-to-Moderate Depression: Randomized Controlled Trial
- PMID: 26813737
- PMCID: PMC4748138
- DOI: 10.2196/mhealth.4231
MoodHacker Mobile Web App With Email for Adults to Self-Manage Mild-to-Moderate Depression: Randomized Controlled Trial
Abstract
Background: Worldwide, depression is rated as the fourth leading cause of disease burden and is projected to be the second leading cause of disability by 2020. Annual depression-related costs in the United States are estimated at US $210.5 billion, with employers bearing over 50% of these costs in productivity loss, absenteeism, and disability. Because most adults with depression never receive treatment, there is a need to develop effective interventions that can be more widely disseminated through new channels, such as employee assistance programs (EAPs), and directly to individuals who will not seek face-to-face care.
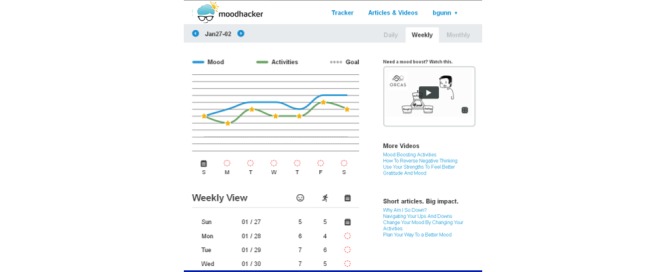
Objective: This study evaluated a self-guided intervention, using the MoodHacker mobile Web app to activate the use of cognitive behavioral therapy (CBT) skills in working adults with mild-to-moderate depression. It was hypothesized that MoodHacker users would experience reduced depression symptoms and negative cognitions, and increased behavioral activation, knowledge of depression, and functioning in the workplace.
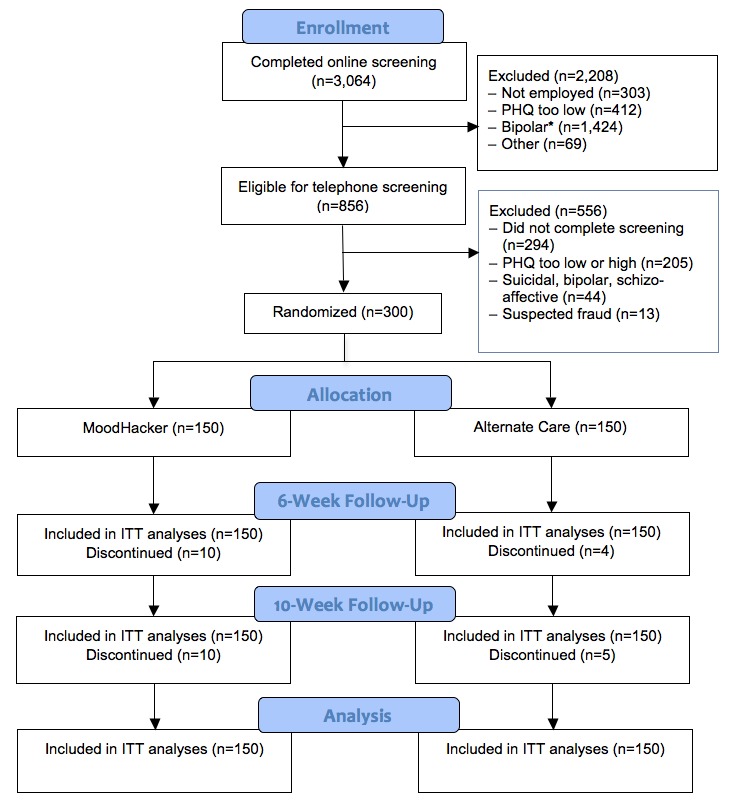
Methods: A parallel two-group randomized controlled trial was conducted with 300 employed adults exhibiting mild-to-moderate depression. Participants were recruited from August 2012 through April 2013 in partnership with an EAP and with outreach through a variety of additional non-EAP organizations. Participants were blocked on race/ethnicity and then randomly assigned within each block to receive, without clinical support, either the MoodHacker intervention (n=150) or alternative care consisting of links to vetted websites on depression (n=150). Participants in both groups completed online self-assessment surveys at baseline, 6 weeks after baseline, and 10 weeks after baseline. Surveys assessed (1) depression symptoms, (2) behavioral activation, (3) negative thoughts, (4) worksite outcomes, (5) depression knowledge, and (6) user satisfaction and usability. After randomization, all interactions with subjects were automated with the exception of safety-related follow-up calls to subjects reporting current suicidal ideation and/or severe depression symptoms.
Results: At 6-week follow-up, significant effects were found on depression, behavioral activation, negative thoughts, knowledge, work productivity, work absence, and workplace distress. MoodHacker yielded significant effects on depression symptoms, work productivity, work absence, and workplace distress for those who reported access to an EAP, but no significant effects on these outcome measures for those without EAP access. Participants in the treatment arm used the MoodHacker app an average of 16.0 times (SD 13.3), totaling an average of 1.3 hours (SD 1.3) of use between pretest and 6-week follow-up. Significant effects on work absence in those with EAP access persisted at 10-week follow-up.
Conclusions: This randomized effectiveness trial found that the MoodHacker app produced significant effects on depression symptoms (partial eta(2) = .021) among employed adults at 6-week follow-up when compared to subjects with access to relevant depression Internet sites. The app had stronger effects for individuals with access to an EAP (partial eta(2) = .093). For all users, the MoodHacker program also yielded greater improvement on work absence, as well as the mediating factors of behavioral activation, negative thoughts, and knowledge of depression self-care. Significant effects were maintained at 10-week follow-up for work absence. General attenuation of effects at 10-week follow-up underscores the importance of extending program contacts to maintain user engagement. This study suggests that light-touch, CBT-based mobile interventions like MoodHacker may be appropriate for implementation within EAPs and similar environments. In addition, it seems likely that supporting MoodHacker users with guidance from counselors may improve effectiveness for those who seek in-person support.
Trial registration: ClinicalTrials.gov NCT02335554; https://clinicaltrials.gov/ct2/show/NCT02335554 (Archived by WebCite at http://www.webcitation.org/6dGXKWjWE).
Keywords: Internet; behavioral activation; cognitive behavioral therapy; computers; depression; mobile apps; positive psychology.
Conflict of interest statement
Conflicts of Interest: Amelia Birney was the study Principal Investigator. She is employed as a Behavioral Scientist at ORCAS, a health innovation and technology company that creates self-management programs to improve physical and emotional well-being. Software development was funded with a Small Business Innovation Research grant, which was designed to stimulate research and product development. Thus, improved versions of MoodHacker are being marketed. Ms Gunn and Mr Russell are no longer employed by ORCAS; they will derive no financial benefit from sales of the MoodHacker app or from publication of this research. Ms Birney and Dr Ary remain employees of ORCAS with some potential for financial benefit from sales of the MoodHacker app.
Figures

References
-
- Kessler RC, Chiu WT, Demler O, Merikangas KR, Walters EE. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005 Jun;62(6):617–627. doi: 10.1001/archpsyc.62.6.617. http://europepmc.org/abstract/MED/15939839 62/6/617 - DOI - PMC - PubMed
-
- Kessler RC. The costs of depression. Psychiatr Clin North Am. 2012 Mar;35(1):1–14. doi: 10.1016/j.psc.2011.11.005. http://europepmc.org/abstract/MED/22370487 S0193-953X(11)00113-4 - DOI - PMC - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
