

Imaging Surrogates of Infiltration Obtained Via Multiparametric Imaging Pattern Analysis Predict Subsequent Location of Recurrence of Glioblastoma
- PMID: 26813856
- PMCID: PMC4853918
- DOI: 10.1227/NEU.0000000000001202
Imaging Surrogates of Infiltration Obtained Via Multiparametric Imaging Pattern Analysis Predict Subsequent Location of Recurrence of Glioblastoma
Abstract
Background: Glioblastoma is an aggressive and highly infiltrative brain cancer. Standard surgical resection is guided by enhancement on postcontrast T1-weighted (T1) magnetic resonance imaging, which is insufficient for delineating surrounding infiltrating tumor.
Objective: To develop imaging biomarkers that delineate areas of tumor infiltration and predict early recurrence in peritumoral tissue. Such markers would enable intensive, yet targeted, surgery and radiotherapy, thereby potentially delaying recurrence and prolonging survival.
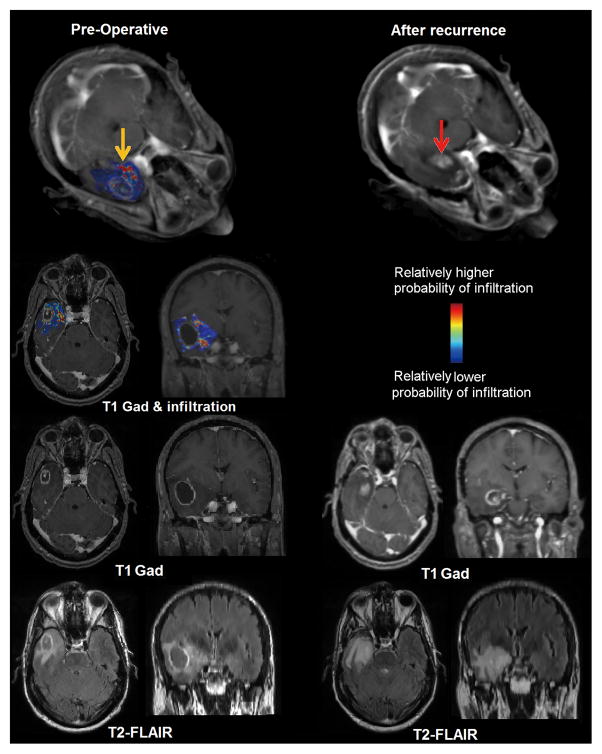
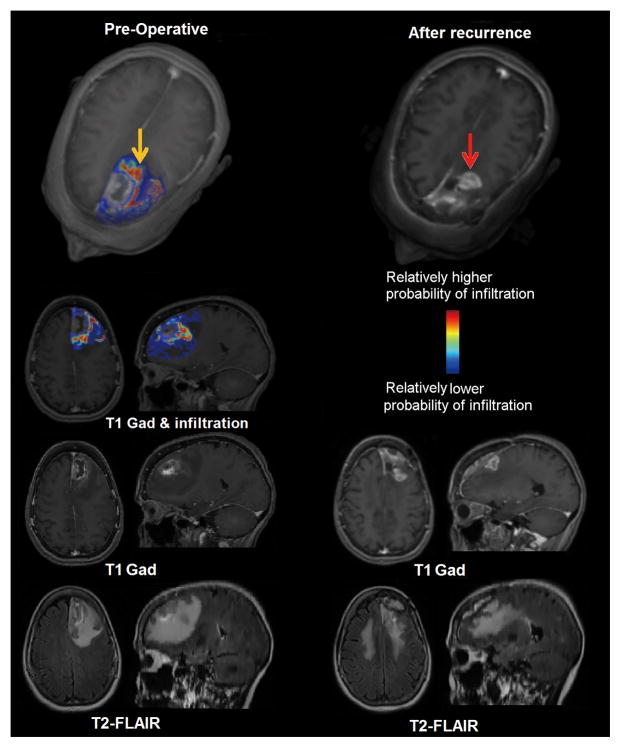
Methods: Preoperative multiparametric magnetic resonance images (T1, T1-gadolinium, T2-weighted, T2-weighted fluid-attenuated inversion recovery, diffusion tensor imaging, and dynamic susceptibility contrast-enhanced magnetic resonance images) from 31 patients were combined using machine learning methods, thereby creating predictive spatial maps of infiltrated peritumoral tissue. Cross-validation was used in the retrospective cohort to achieve generalizable biomarkers. Subsequently, the imaging signatures learned from the retrospective study were used in a replication cohort of 34 new patients. Spatial maps representing the likelihood of tumor infiltration and future early recurrence were compared with regions of recurrence on postresection follow-up studies with pathology confirmation.
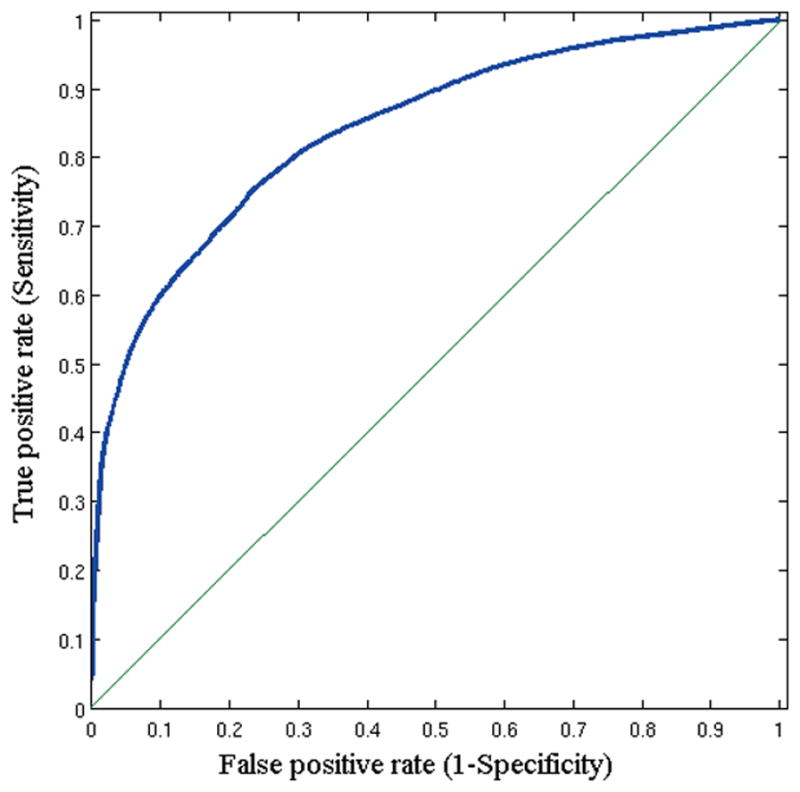
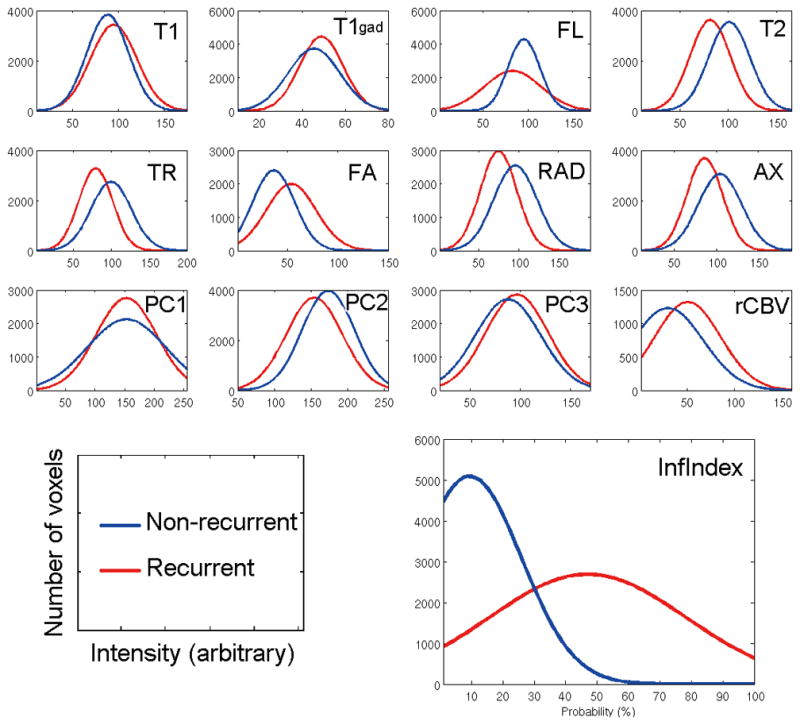
Results: This technique produced predictions of early recurrence with a mean area under the curve of 0.84, sensitivity of 91%, specificity of 93%, and odds ratio estimates of 9.29 (99% confidence interval: 8.95-9.65) for tissue predicted to be heavily infiltrated in the replication study. Regions of tumor recurrence were found to have subtle, yet fairly distinctive multiparametric imaging signatures when analyzed quantitatively by pattern analysis and machine learning.
Conclusion: Visually imperceptible imaging patterns discovered via multiparametric pattern analysis methods were found to estimate the extent of infiltration and location of future tumor recurrence, paving the way for improved targeted treatment.
Figures
References
-
- Yang I, Aghi MK. New advances that enable identification of glioblastoma recurrence. Nature Reviews Clinical Oncology. 2009;6(11):648–657. - PubMed
-
- Brandsma D, Stalpers L, Taal W, Sminia P, van den Bent MJ. Clinical features, mechanisms, and management of pseudoprogression in malignant gliomas. The lancet oncology. 2008;9(5):453–461. - PubMed
-
- Sanai N, Polley M-Y, McDermott MW, Parsa AT, Berger MS. An extent of resection threshold for newly diagnosed glioblastomas: Clinical article. Journal of neurosurgery. 2011;115(1):3–8. - PubMed
-
- Stupp R, Mason WP, Van Den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. New England Journal of Medicine. 2005;352(10):987–996. - PubMed
-
- Heesters M, Wijrdeman H, Struikmans H, Witkamp T, Moerland M. Brain tumor delineation based on CT and MR imaging. Implications for radiotherapy treatment planning. Strahlentherapie und Onkologie: Organ der Deutschen Rontgengesellschaft... [et al] 1993;169(12):729–733. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
