

Mechanisms of resistance in castration-resistant prostate cancer (CRPC)
- PMID: 26814148
- PMCID: PMC4708226
- DOI: 10.3978/j.issn.2223-4683.2015.05.02
Mechanisms of resistance in castration-resistant prostate cancer (CRPC)
Abstract
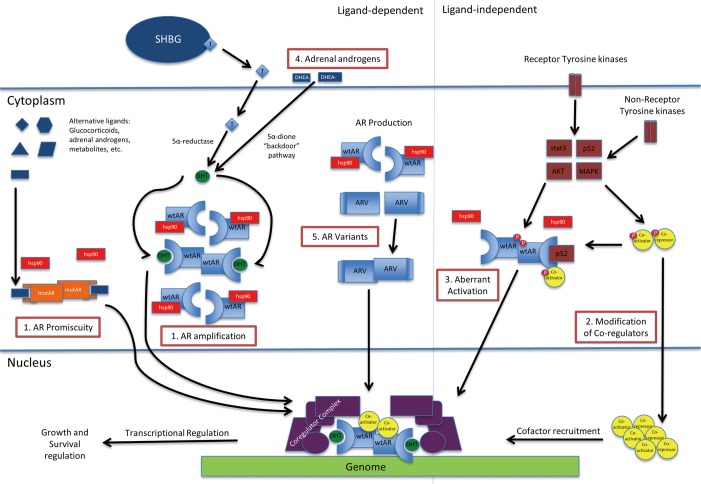
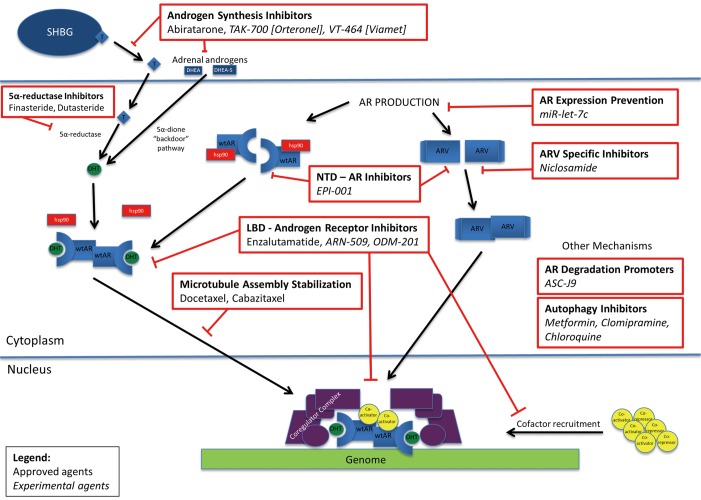
Despite advances in prostate cancer diagnosis and management, morbidity from prostate cancer remains high. Approximately 20% of men present with advanced or metastatic disease, while 29,000 men continue to die of prostate cancer each year. Androgen deprivation therapy (ADT) has been the standard of care for initial management of advanced or metastatic prostate cancer since Huggins and Hodges first introduced the concept of androgen-dependence in 1972, but progression to castration-resistant prostate cancer (CRPC) occurs within 2-3 years of initiation of ADT. CRPC, previously defined as hormone-refractory prostate cancer, is now understood to still be androgen dependent. Multiple mechanisms of resistance help contribute to the progression to castration resistant disease, and the androgen receptor (AR) remains an important driver in this progression. These mechanisms include AR amplification and hypersensitivity, AR mutations leading to promiscuity, mutations in coactivators/corepressors, androgen-independent AR activation, and intratumoral and alternative androgen production. More recently, identification of AR variants (ARVs) has been established as another mechanism of progression to CRPC. Docetaxel chemotherapy has historically been the first-line treatment for CRPC, but in recent years, newer agents have been introduced that target some of these mechanisms of resistance, thereby providing additional survival benefit. These include AR signaling inhibitors such as enzalutamide (Xtandi, ENZA, MDV-3100) and CYP17A1 inhibitors such as abiraterone acetate (Zytiga). Ultimately, these agents will also fail to suppress CRPC. While some of the mechanisms by which these agents fail are unique, many share similarities to the mechanisms contributing to CRPC progression. Understanding these mechanisms of resistance to ADT and currently approved CRPC treatments will help guide future research into targeted therapies.
Keywords: Castration-resistant; disease progression; drug resistance; prostatic neoplasms.
Conflict of interest statement
Figures
References
-
- Siegel R, Ma J, Zou Z, et al. Cancer statistics, 2014. CA Cancer J Clin 2014;64:9-29. - PubMed
-
- Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer 2013;49:1374-403. - PubMed
-
- Studer UE, Hauri D, Hanselmann S, et al. Immediate versus deferred hormonal treatment for patients with prostate cancer who are not suitable for curative local treatment: results of the randomized trial SAKK 08/88. J Clin Oncol 2004;22:4109-18. - PubMed
-
- Hughes IA, Davies JD, Bunch TI, et al. Androgen insensitivity syndrome. Lancet 2012;380:1419-28. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials