

Steatohepatitis and liver fibrosis are predicted by the characteristics of very low density lipoprotein in nonalcoholic fatty liver disease
- PMID: 26815314
- PMCID: PMC4942367
- DOI: 10.1111/liv.13076
Steatohepatitis and liver fibrosis are predicted by the characteristics of very low density lipoprotein in nonalcoholic fatty liver disease
Abstract
Background & aims: A major challenge in the management of nonalcoholic fatty liver disease (NAFLD) is to identify patients with nonalcoholic steatohepatitis (NASH) and early liver fibrosis. The progression of NAFLD is accompanied by distinctive changes in very low density lipoprotein (VLDL), a lipoprotein particle produced exclusively in the liver. Herein, we sought to determine the characteristics of VLDL profiles associated with NASH and liver fibrosis.
Methods: We evaluated VLDL profiles of 128 patients from a single centre NAFLD registry, and examined VLDL size, total and subclass VLDL concentrations in relation to NAFLD activity score (NAS), steatohepatitis and liver fibrosis as determined by liver biopsy.
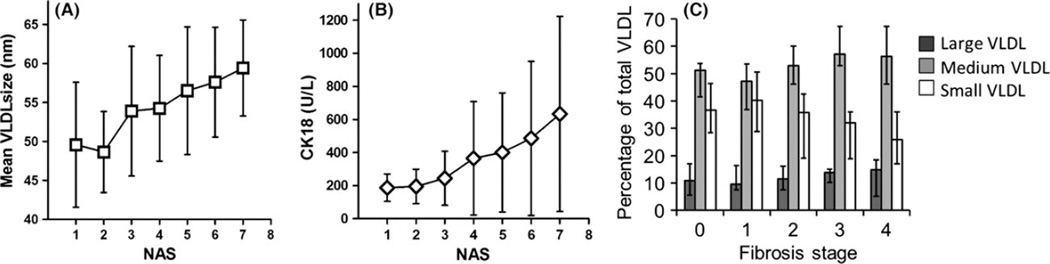
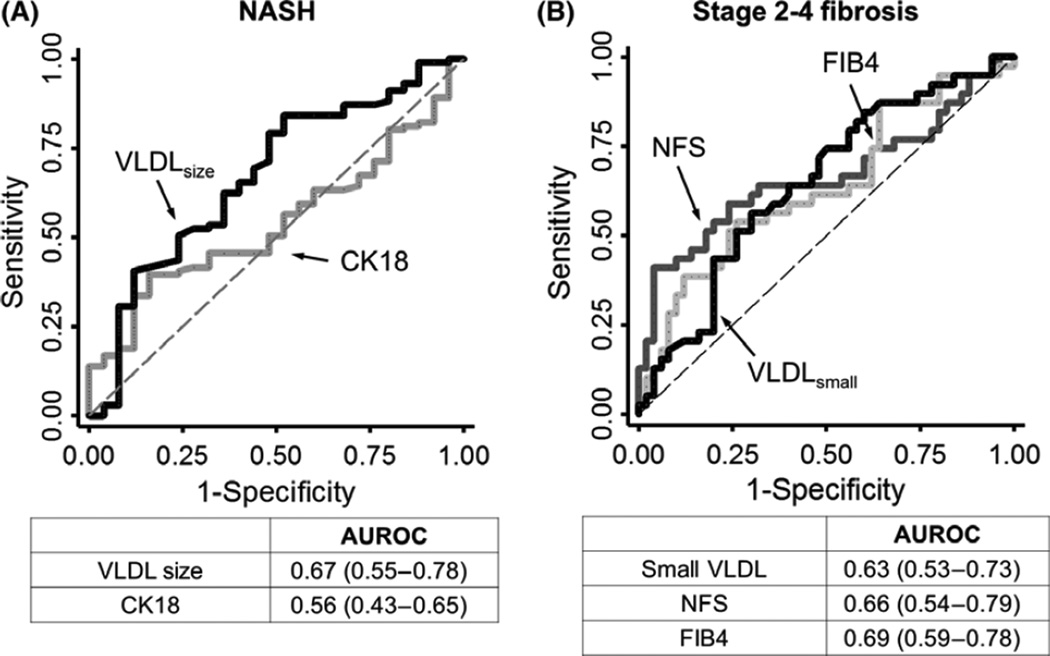
Results: A near linear relationship was observed between mean VLDL particle size and NAFLD activity score (NAS). In multivariate models, VLDL particle size was significantly associated with both NAS and NASH, after adjustment for BMI and diabetes. A decrease in small VLDL particle concentration was associated with more advanced liver fibrosis. In receiver operative characteristic analyses, mean VLDL size performed similarly to cytokeratin 18 in predicting NASH, whereas small VLDL particle concentration had similar performance to NAFLD fibrosis score in predicting stage 2 or above liver fibrosis.
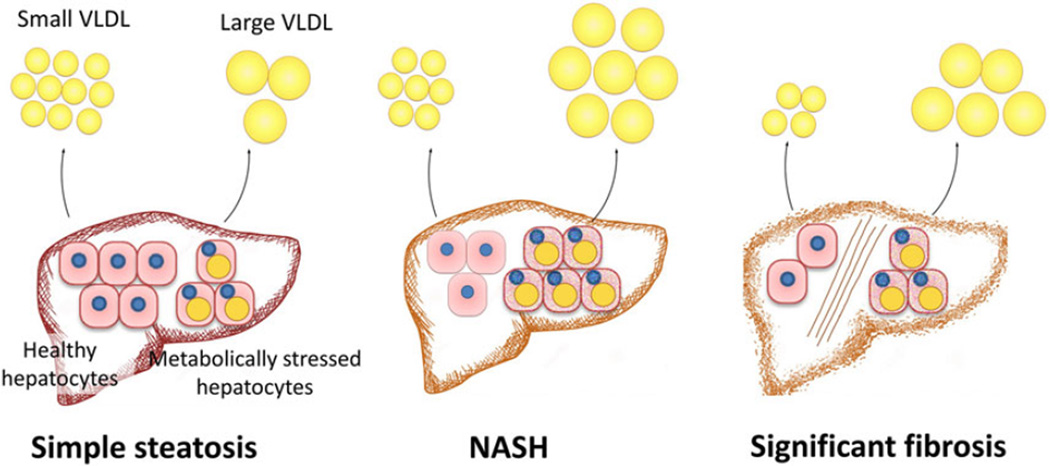
Conclusions: The increase in mean VLDL size in NASH and decrease in small VLDL particle concentration in liver fibrosis likely reflect changes in the number and state of hepatocytes associated with NASH and fibrosis. In addition to its value in risk stratification of cardiovascular diseases, circulating VLDL profile may provide information for the staging of NAFLD disease severity.
Keywords: lipoprotein metabolism; nonalcoholic fatty liver disease; nonalcoholic steatohepatitis; very low density lipoprotein.
© 2016 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Figures
Similar articles
-
Serum cytokeratin-18 fragment levels as noninvasive marker of nonalcoholic steatohepatitis in the chilean population.Gastroenterol Hepatol. 2017 Jun-Jul;40(6):388-394. doi: 10.1016/j.gastrohep.2017.02.009. Epub 2017 Mar 28. Gastroenterol Hepatol. 2017. PMID: 28359548 English, Spanish.
-
Association between triglyceride glucose-body mass index and the staging of non-alcoholic steatohepatitis and fibrosis in patients with non-alcoholic fatty liver disease.Ann Med. 2024 Dec;56(1):2409342. doi: 10.1080/07853890.2024.2409342. Epub 2024 Sep 30. Ann Med. 2024. PMID: 39348274 Free PMC article.
-
Nonalcoholic fatty liver disease associated with metabolic syndrome: Influence of liver fibrosis stages on characteristics of very low-density lipoproteins.Clin Chim Acta. 2017 Oct;473:1-8. doi: 10.1016/j.cca.2017.08.006. Epub 2017 Aug 9. Clin Chim Acta. 2017. PMID: 28802640
-
Liver fibrosis markers of nonalcoholic steatohepatitis.World J Gastroenterol. 2015 Jun 28;21(24):7427-35. doi: 10.3748/wjg.v21.i24.7427. World J Gastroenterol. 2015. PMID: 26139988 Free PMC article. Review.
-
Histopathology of nonalcoholic fatty liver disease/nonalcoholic steatohepatitis.World J Gastroenterol. 2014 Nov 14;20(42):15539-48. doi: 10.3748/wjg.v20.i42.15539. World J Gastroenterol. 2014. PMID: 25400438 Free PMC article. Review.
Cited by
-
The Role of Lipid Profile as an Independent Predictor of Non-alcoholic Steatosis and Steatohepatitis in Morbidly Obese Patients.Front Cardiovasc Med. 2021 May 31;8:682352. doi: 10.3389/fcvm.2021.682352. eCollection 2021. Front Cardiovasc Med. 2021. PMID: 34136549 Free PMC article.
-
VITAMIN D DEFICIENCY, A NONINVASIVE MARKER OF STEATOHEPATITIS IN PATIENTS WITH OBESITY AND BIOPSY PROVEN NONALCOHOLIC FATTY LIVER DISEASE.Acta Endocrinol (Buchar). 2018 Jan-Mar;14(1):76-84. doi: 10.4183/aeb.2018.76. Acta Endocrinol (Buchar). 2018. PMID: 31149239 Free PMC article.
-
Quantitative digital pathology reveals association of cell-specific PNPLA3 transcription with NAFLD disease activity.JHEP Rep. 2019 Jun 8;1(3):199-202. doi: 10.1016/j.jhepr.2019.05.007. eCollection 2019 Sep. JHEP Rep. 2019. PMID: 32039370 Free PMC article.
-
Serum Activity of Macrophage-Derived Adenosine Deaminase 2 Is Associated With Liver Fibrosis in Nonalcoholic Fatty Liver Disease.Clin Gastroenterol Hepatol. 2018 Jul;16(7):1170-1172. doi: 10.1016/j.cgh.2017.11.028. Epub 2017 Nov 21. Clin Gastroenterol Hepatol. 2018. PMID: 29170098 Free PMC article. No abstract available.
-
Lipoprotein A, combined with alanine aminotransferase and aspartate aminotransferase, contributes to predicting the occurrence of NASH: a cross-sectional study.Lipids Health Dis. 2020 Jun 11;19(1):134. doi: 10.1186/s12944-020-01310-x. Lipids Health Dis. 2020. PMID: 32527258 Free PMC article.
References
-
- Afdhal NH. Management of nonalcoholic fatty liver disease: a 60-year-old man with probable nonalcoholic fatty liver disease: weight reduction, liver biopsy, or both? JAMA. 2012;308:608–616. - PubMed
-
- Younossi ZM, Stepanova M, Afendy M, et al. Changes in the prevalence of the most common causes of chronic liver diseases in the United States from 1988 to 2008. Clin Gastroenterol Hepatol. 2011;9:524–530. e1. quiz e60. - PubMed
-
- Adams LA, Lymp JF, St Sauver J, et al. The natural history of nonalcoholic fatty liver disease: a population-based cohort study. Gastroenterology. 2005;129:113–121. - PubMed
-
- Rockey DC, Caldwell SH, Goodman ZD, Nelson RC, Smith AD American Association for the Study of Liver D. Liver biopsy. Hepatology. 2009;49:1017–1044. - PubMed
-
- Castera L, Vilgrain V, Angulo P. Noninvasive evaluation of NAFLD. Nat Rev Gastroenterol Hepatol. 2013;10:666–675. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
