

Diffuse Optical Characterization of the Healthy Human Thyroid Tissue and Two Pathological Case Studies
- PMID: 26815533
- PMCID: PMC4731400
- DOI: 10.1371/journal.pone.0147851
Diffuse Optical Characterization of the Healthy Human Thyroid Tissue and Two Pathological Case Studies
Abstract
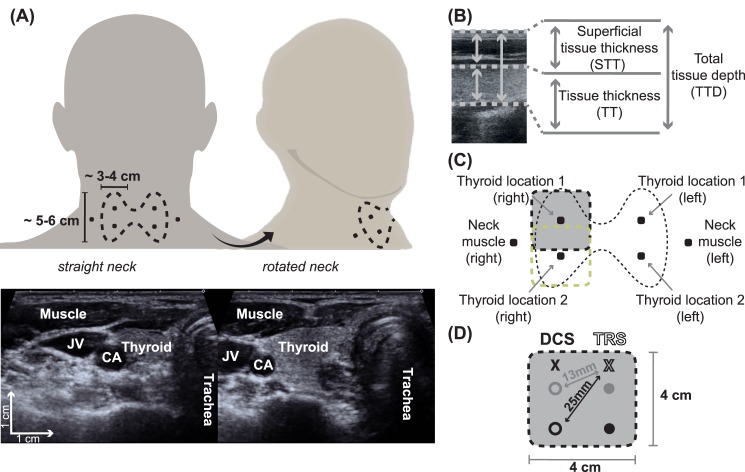
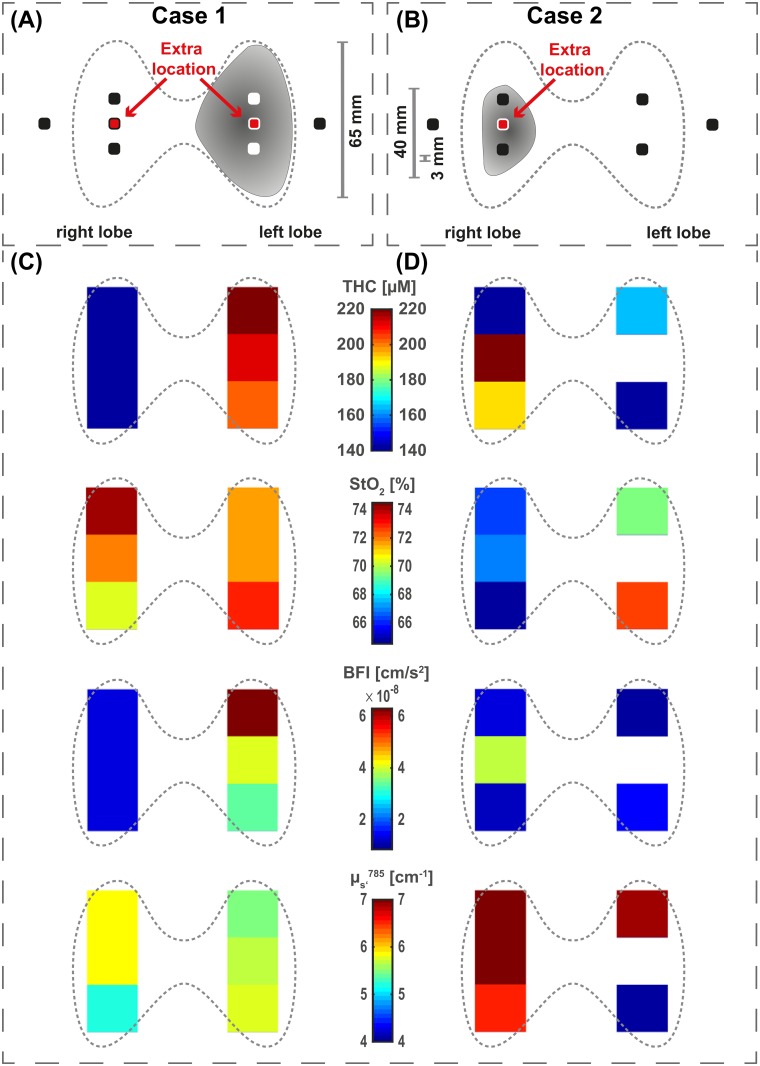
The in vivo optical and hemodynamic properties of the healthy (n = 22) and pathological (n = 2) human thyroid tissue were measured non-invasively using a custom time-resolved spectroscopy (TRS) and diffuse correlation spectroscopy (DCS) system. Medical ultrasound was used to guide the placement of the hand-held hybrid optical probe. TRS measured the absorption and reduced scattering coefficients (μa, μs') at three wavelengths (690, 785 and 830 nm) to derive total hemoglobin concentration (THC) and oxygen saturation (StO2). DCS measured the microvascular blood flow index (BFI). Their dependencies on physiological and clinical parameters and positions along the thyroid were investigated and compared to the surrounding sternocleidomastoid muscle. The THC in the thyroid ranged from 131.9 μM to 144.8 μM, showing a 25-44% increase compared to the surrounding sternocleidomastoid muscle tissue. The blood flow was significantly higher in the thyroid (BFIthyroid = 16.0 × 10-9 cm2/s) compared to the muscle (BFImuscle = 7.8 × 10-9 cm2/s), while StO2 showed a small (StO2, muscle = 63.8% to StO2, thyroid = 68.4%), yet significant difference. Two case studies with thyroid nodules underwent the same measurement protocol prior to thyroidectomy. Their THC and BFI reached values around 226.5 μM and 62.8 × 10-9 cm2/s respectively showing a clear contrast to the nodule-free thyroid tissue as well as the general population. The initial characterization of the healthy and pathologic human thyroid tissue lays the ground work for the future investigation on the use of diffuse optics in thyroid cancer screening.
Conflict of interest statement
Figures
Similar articles
-
Impact of changes in tissue optical properties on near-infrared diffuse correlation spectroscopy measures of skeletal muscle blood flow.J Appl Physiol (1985). 2021 Apr 1;130(4):1183-1195. doi: 10.1152/japplphysiol.00857.2020. Epub 2021 Feb 11. J Appl Physiol (1985). 2021. PMID: 33571054 Free PMC article.
-
In vivocharacterization of the optical and hemodynamic properties of the human sternocleidomastoid muscle through ultrasound-guided hybrid near-infrared spectroscopies.Physiol Meas. 2023 Dec 26;44(12). doi: 10.1088/1361-6579/ad133a. Physiol Meas. 2023. PMID: 38061053
-
Malignant thyroid nodules: comparison between color Doppler diagnosis and histological examination of surgical samples.Chir Ital. 2002 Sep-Oct;54(5):643-7. Chir Ital. 2002. PMID: 12469461
-
Management of the solitary thyroid nodule.Oncologist. 2008 Feb;13(2):105-12. doi: 10.1634/theoncologist.2007-0212. Oncologist. 2008. PMID: 18305054 Review.
-
Thyroid nodules; interpretation and importance of fine-needle aspiration (FNA) for the clinician - practical considerations.Surg Oncol. 2010 Dec;19(4):e130-9. doi: 10.1016/j.suronc.2010.06.003. Surg Oncol. 2010. PMID: 20620044 Review.
Cited by
-
Transcranial optical monitoring for detecting intracranial pressure alterations in children with benign external hydrocephalus: a proof-of-concept study.Neurophotonics. 2022 Oct;9(4):045005. doi: 10.1117/1.NPh.9.4.045005. Epub 2022 Nov 17. Neurophotonics. 2022. PMID: 36405998 Free PMC article.
-
Comparison of cerebral metabolic rate of oxygen, blood flow, and bispectral index under general anesthesia.Neurophotonics. 2023 Jan;10(1):015006. doi: 10.1117/1.NPh.10.1.015006. Epub 2023 Mar 6. Neurophotonics. 2023. PMID: 36911206 Free PMC article.
-
The LUCA device: a multi-modal platform combining diffuse optics and ultrasound imaging for thyroid cancer screening.Biomed Opt Express. 2021 May 14;12(6):3392-3409. doi: 10.1364/BOE.416561. eCollection 2021 Jun 1. Biomed Opt Express. 2021. PMID: 34221667 Free PMC article.
-
Difference imaging from single measurements in diffuse optical tomography: a deep learning approach.J Biomed Opt. 2022 Aug;27(8):086003. doi: 10.1117/1.JBO.27.8.086003. J Biomed Opt. 2022. PMID: 36008881 Free PMC article.
-
Recipes for diffuse correlation spectroscopy instrument design using commonly utilized hardware based on targets for signal-to-noise ratio and precision.Biomed Opt Express. 2021 May 11;12(6):3265-3281. doi: 10.1364/BOE.423071. eCollection 2021 Jun 1. Biomed Opt Express. 2021. PMID: 34221659 Free PMC article.
References
-
- Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL, Mandel SJ, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association (ATA) guidelines taskforce on thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19(11):1167–1214. 10.1089/thy.2009.0110 - DOI - PubMed
-
- Gharib H, Papini E, Paschke R, Duick D, Valcavi R, Hegedüs L, et al. American Association of Clinical Endocrinologists, Associazione Medici Endocrinologi, and European Thyroid Association medical guidelines for clinical practice for the diagnosis and management of thyroid nodules. Endocrine Practice. 2010;16(Supplement 1):1–43. 10.4158/10024.GL - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
