

Five-Year Mortality and Hospital Costs Associated with Surviving Intensive Care
- PMID: 26815887
- PMCID: PMC5003217
- DOI: 10.1164/rccm.201511-2234OC
Five-Year Mortality and Hospital Costs Associated with Surviving Intensive Care
Abstract
Rationale: Survivors of critical illness experience significant morbidity, but the impact of surviving the intensive care unit (ICU) has not been quantified comprehensively at a population level.
Objectives: To identify factors associated with increased hospital resource use and to ascertain whether ICU admission was associated with increased mortality and resource use.
Methods: Matched cohort study and pre/post-analysis using national linked data registries with complete population coverage. The population consisted of patients admitted to all adult general ICUs during 2005 and surviving to hospital discharge, identified from the Scottish Intensive Care Society Audit Group registry, matched (1:1) with similar hospital control subjects. Five-year outcomes included mortality and hospital resource use. Confounder adjustment was based on multivariable regression and pre/post within-individual analyses.
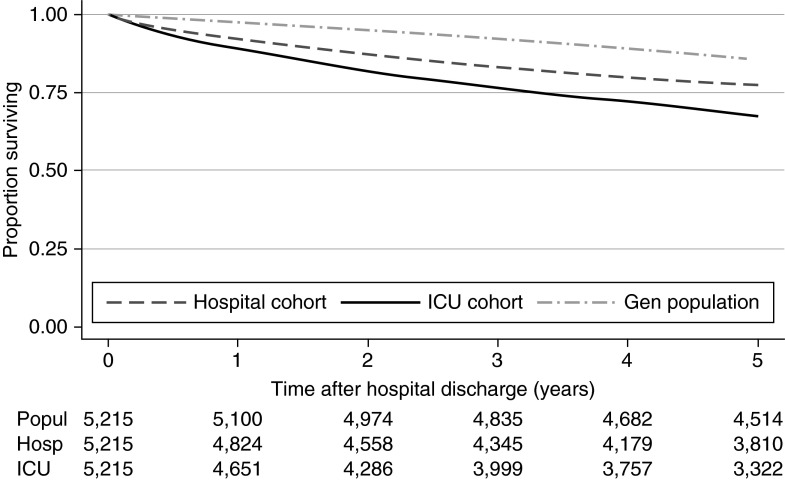
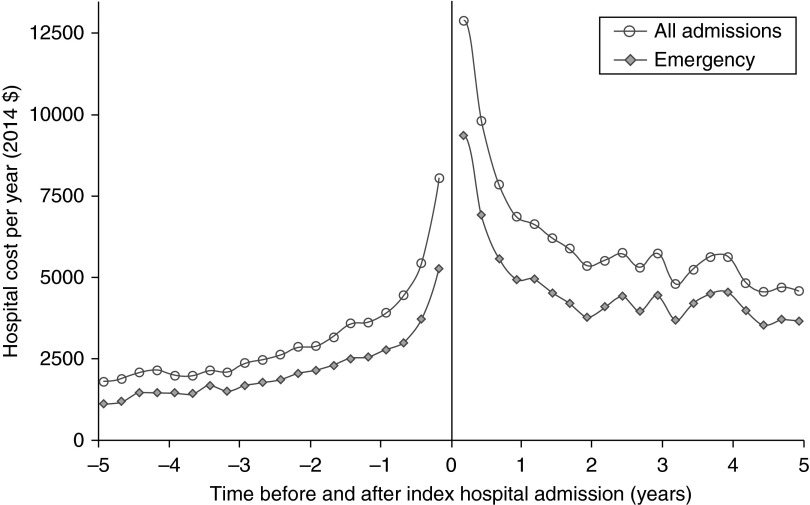
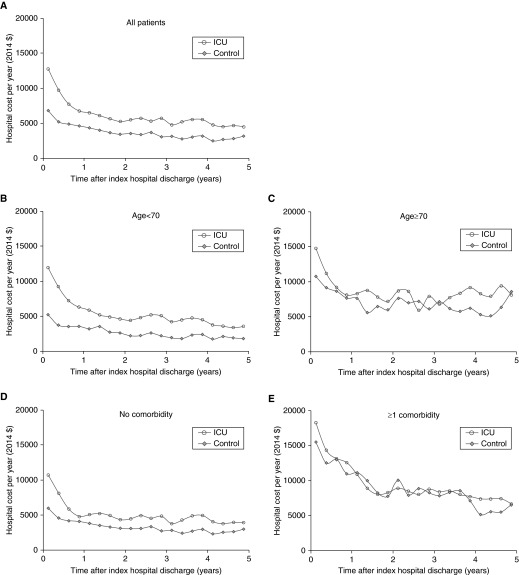
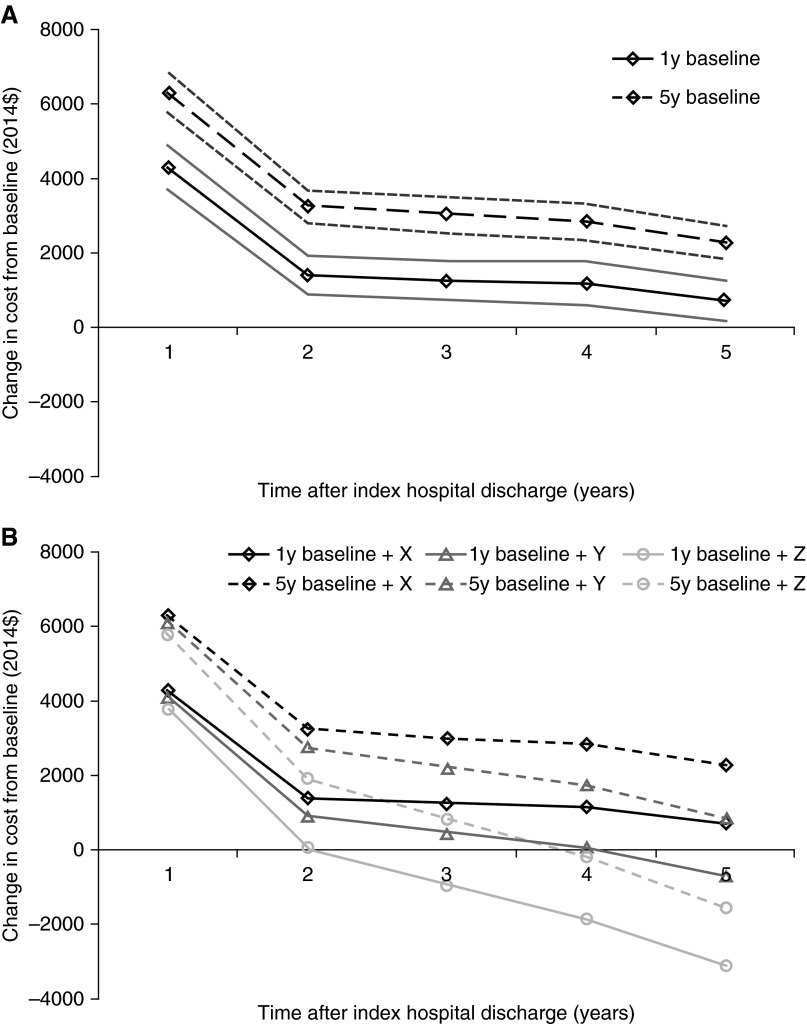
Measurements and main results: Of 7,656 ICU patients, 5,259 survived to hospital discharge (5,215 [99.2%] matched to hospital control subjects). Factors present before ICU admission (comorbidities/pre-ICU hospitalizations) were stronger predictors of hospital resource use than acute illness factors. In the 5 years after the initial hospital discharge, compared with hospital control subjects, the ICU cohort had higher mortality (32.3% vs. 22.7%; hazard ratio, 1.33; 95% confidence interval, 1.22-1.46; P < 0.001), used more hospital resources (mean hospital admission rate, 4.8 vs. 3.3/person/5 yr), and had 51% higher mean 5-year hospital costs ($25,608 vs. $16,913/patient). Increased resource use persisted after confounder adjustment (P < 0.001) and using pre/post-analyses (P < 0.001). Excess resource use and mortality were greatest for younger patients without significant comorbidity.
Conclusions: This complete, national study demonstrates that ICU survivorship is associated with higher 5-year mortality and hospital resource use than hospital control subjects, representing a substantial burden on individuals, caregivers, and society.
Keywords: hospital costs; hospital readmission; intensive care; mortality; registries.
Figures
References
-
- Desai SV, Law TJ, Needham DM. Long-term complications of critical care. Crit Care Med. 2011;39:371–379. - PubMed
-
- Stevens RD, Dowdy DW, Michaels RK, Mendez-Tellez PA, Pronovost PJ, Needham DM. Neuromuscular dysfunction acquired in critical illness: a systematic review. Intensive Care Med. 2007;33:1876–1891. - PubMed
-
- Herridge MS, Tansey CM, Matté A, Tomlinson G, Diaz-Granados N, Cooper A, Guest CB, Mazer CD, Mehta S, Stewart TE, et al. Canadian Critical Care Trials Group. Functional disability 5 years after acute respiratory distress syndrome. N Engl J Med. 2011;364:1293–1304. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
