

Host Factors and Biomarkers Associated with Poor Outcomes in Adults with Invasive Pneumococcal Disease
- PMID: 26815915
- PMCID: PMC4731463
- DOI: 10.1371/journal.pone.0147877
Host Factors and Biomarkers Associated with Poor Outcomes in Adults with Invasive Pneumococcal Disease
Erratum in
-
Correction: Host Factors and Biomarkers Associated with Poor Outcomes in Adults with Invasive Pneumococcal Disease.PLoS One. 2016 Mar 31;11(3):e0153109. doi: 10.1371/journal.pone.0153109. eCollection 2016. PLoS One. 2016. PMID: 27031245 Free PMC article. No abstract available.
Abstract
Background: Invasive pneumococcal disease (IPD) causes considerable morbidity and mortality. We aimed to identify host factors and biomarkers associated with poor outcomes in adult patients with IPD in Japan, which has a rapidly-aging population.
Methods: In a large-scale surveillance study of 506 Japanese adults with IPD, we investigated the role of host factors, disease severity, biomarkers based on clinical laboratory data, treatment regimens, and bacterial factors on 28-day mortality.
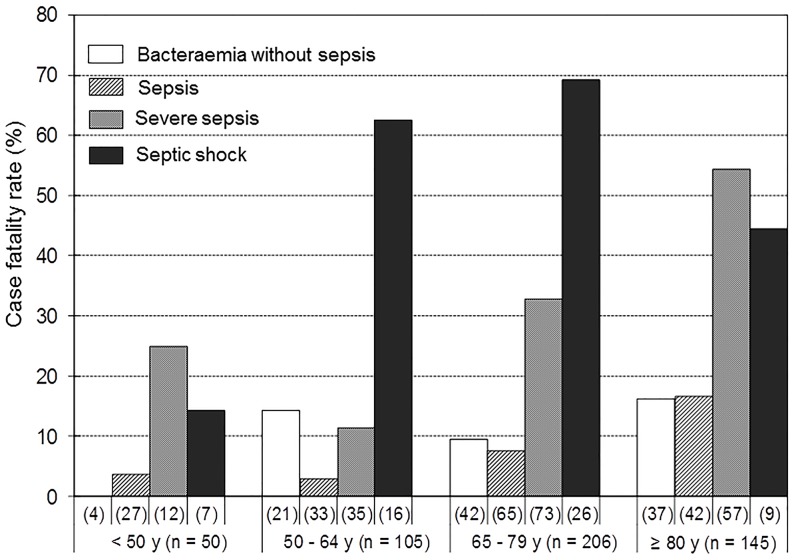
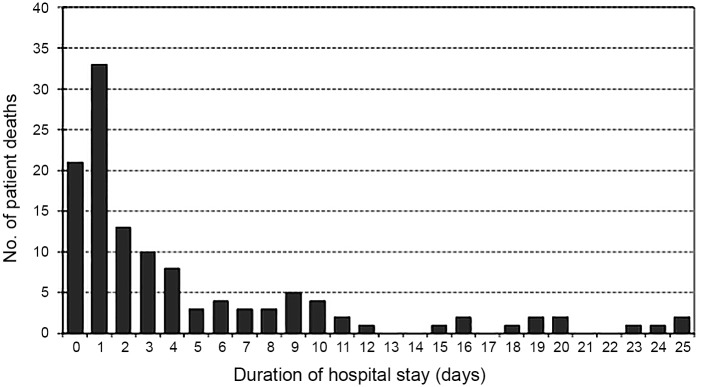
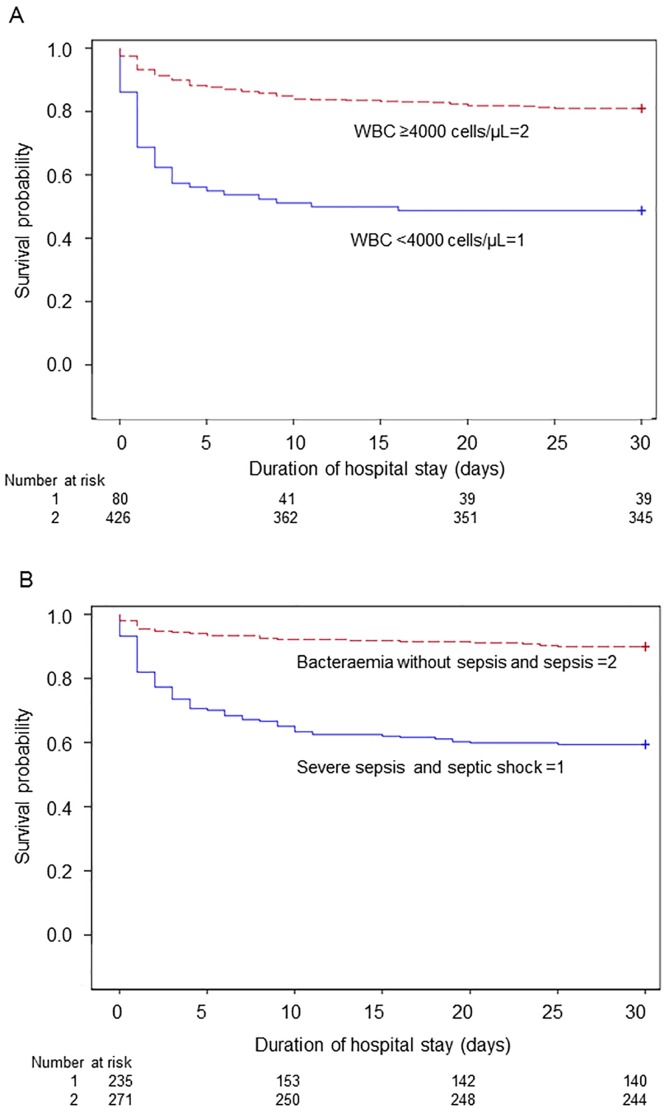
Results: Overall mortality was 24.1%, and the mortality rate increased from 10.0% in patients aged ˂50 years to 33.1% in patients aged ≥80 years. Disease severity also increased 28-day mortality, from 12.5% among patients with bacteraemia without sepsis to 35.0% in patients with severe sepsis and 56.9% with septic shock. The death rate within 48 hours after admission was high at 54.9%. Risk factors for mortality identified by multivariate analysis were as follows: white blood cell (WBC) count <4000 cells/μL (odds ratio [OR], 6.9; 95% confidence interval [CI], 3.7-12.8, p < .001); age ≥80 years (OR, 6.5; 95% CI, 2.0-21.6, p = .002); serum creatinine ≥2.0 mg/dL (OR, 4.5; 95% CI, 2.5-8.1, p < .001); underlying liver disease (OR, 3.5; 95% CI, 1.6-7.8, p = .002); mechanical ventilation (OR, 3.0; 95% CI, 1.7-5.6, p < .001); and lactate dehydrogenase ≥300 IU/L (OR, 2.4; 95% CI, 1.4-4.0, p = .001). Pneumococcal serotype and drug resistance were not associated with poor outcomes.
Conclusions: Host factors, disease severity, and biomarkers, especially WBC counts and serum creatinine, were more important determinants of mortality than bacterial factors.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
