

Quantitative assessment of atherosclerotic plaques on (18)F-FDG PET/MRI: comparison with a PET/CT hybrid system
- PMID: 26816195
- PMCID: PMC4906060
- DOI: 10.1007/s00259-016-3308-6
Quantitative assessment of atherosclerotic plaques on (18)F-FDG PET/MRI: comparison with a PET/CT hybrid system
Erratum in
-
Erratum to: Quantitative assessment of atherosclerotic plaques on 18F-FDG PET/MRI: comparison with a PET/CT hybrid system.Eur J Nucl Med Mol Imaging. 2016 Jul;43(8):1569. doi: 10.1007/s00259-016-3375-8. Eur J Nucl Med Mol Imaging. 2016. PMID: 27000852 Free PMC article. No abstract available.
Abstract
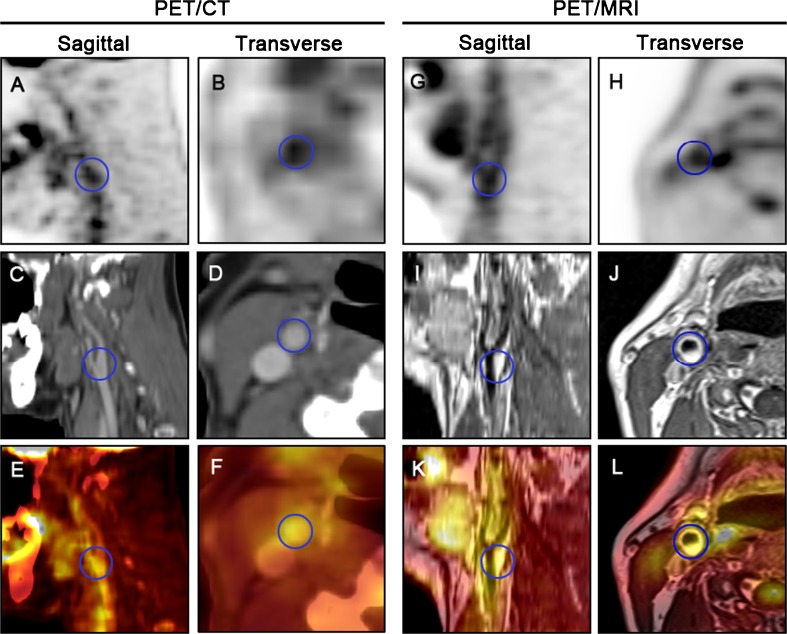
Purpose: PET with (18)F-FDG has the potential to assess vascular macrophage metabolism. (18)F-FDG is most often used in combination with contrast-enhanced CT to localize increased metabolism to specific arterial lesions. Novel (18)F-FDG PET/MRI hybrid imaging shows high potential for the combined evaluation of atherosclerotic plaques, due to the superior morphological conspicuity of plaque lesions. The purpose of this study was to evaluate the reliability and accuracy of (18)F-FDG PET/MRI uptake quantification compared to PET/CT as a reference standard in patients with carotid atherosclerotic plaques.
Methods: The study group comprised 34 consecutive oncological patients with carotid plaques who underwent both PET/CT and PET/MRI with (18)F-FDG on the same day. The presence of atherosclerotic plaques was confirmed by 3 T MRI scans. Maximum standardized uptake values (SUVmax) for carotid plaque lesions and the average SUV of the blood pool within the adjacent internal jugular vein were determined and target-to-blood ratios (TBRs, plaque to blood pool) were calculated.
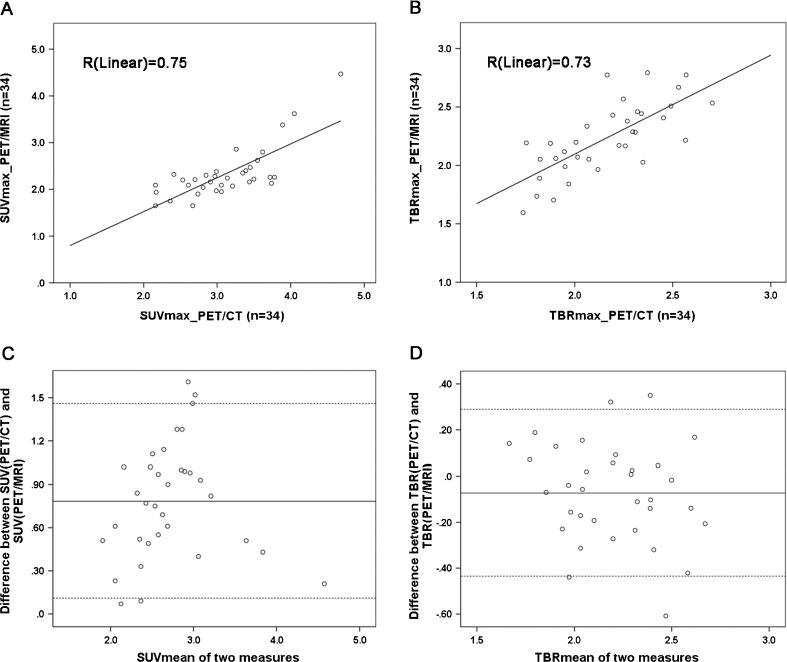
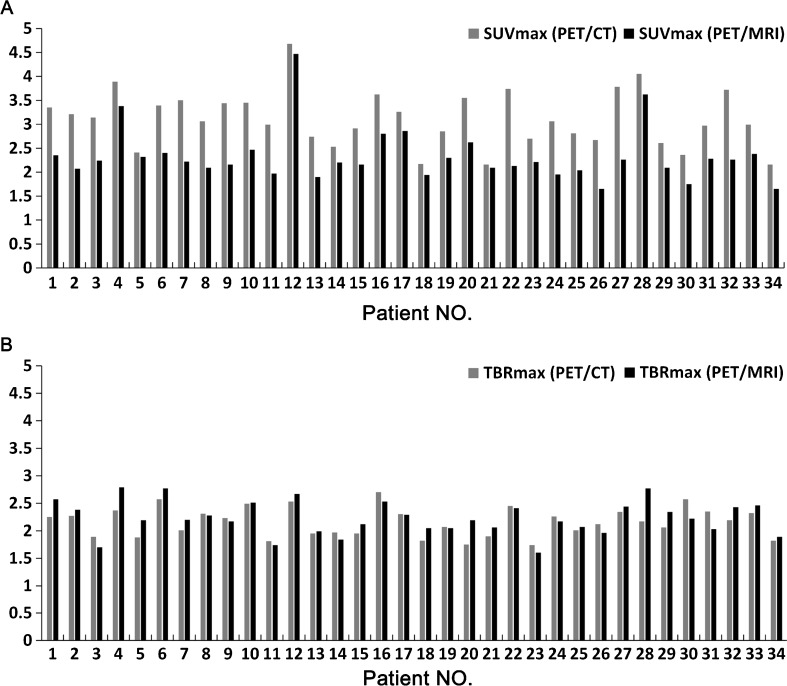
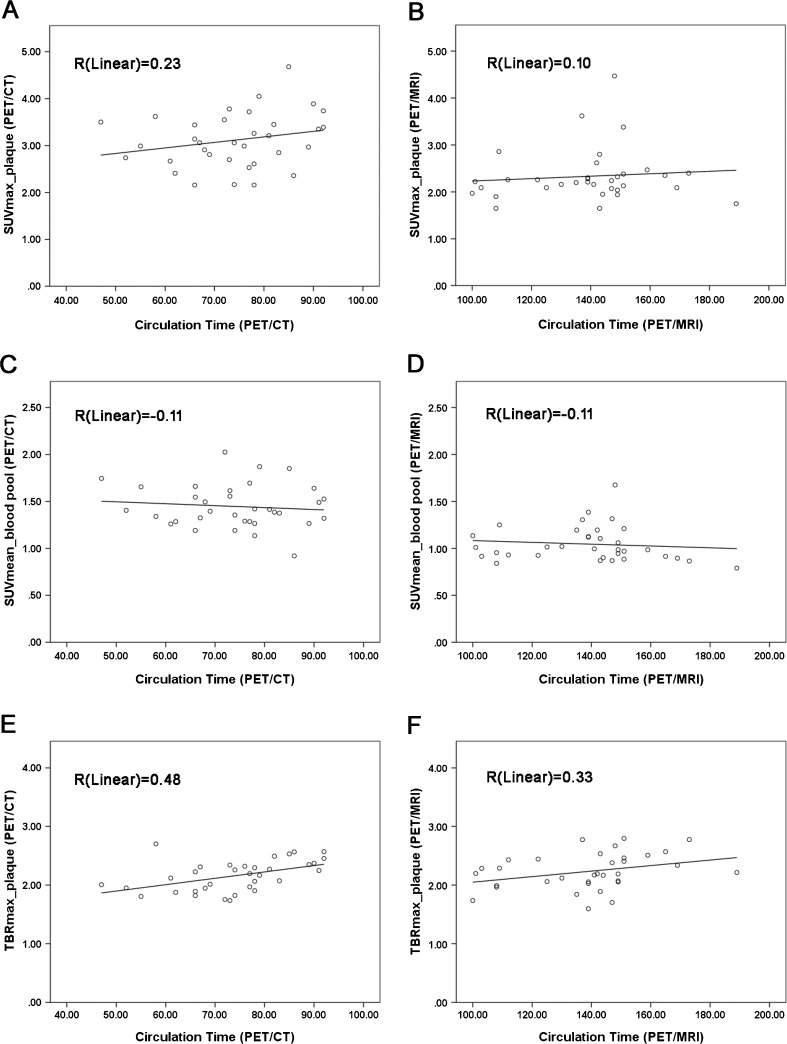
Results: Atherosclerotic lesions with maximum colocalized focal FDG uptake were assessed in each patient. SUVmax values of carotid plaque lesions were significantly lower on PET/MRI than on PET/CT (2.3 ± 0.6 vs. 3.1 ± 0.6; P < 0.01), but were significantly correlated between PET/CT and PET/MRI (Spearman's r = 0.67, P < 0.01). In contrast, TBRmax values of plaque lesions were similar on PET/MRI and on PET/CT (2.2 ± 0.3 vs. 2.2 ± 0.3; P = 0.4), and again were significantly correlated between PET/MRI and PET/CT (Spearman's r = 0.73, P < 0.01). Considering the increasing trend in SUVmax and TBRmax values from early to delayed imaging time-points on PET/CT and PET/MRI, respectively, with continuous clearance of radioactivity from the blood, a slight underestimation of TBRmax values may also be expected with PET/MRI compared with PET/CT.
Conclusion: SUVmax and TBRmax values are widely accepted reference parameters for estimation of the radioactivity of atherosclerotic plaques on PET/CT. However, due to a systematic underestimation of SUVmax and TBRmax with PET/MRI, the optimal cut-off values indicating the presence of inflamed plaque tissue need to be newly defined for PET/MRI.
Keywords: 18F-FDG; Atherosclerosis; Carotid plaque; Inflammation; PET/CT; PET/MRI.
Figures
Similar articles
-
[18F]-Fluorodeoxyglucose PET/CT imaging as a marker of carotid plaque inflammation: Comparison to immunohistology and relationship to acuity of events.Int J Cardiol. 2018 Nov 15;271:378-386. doi: 10.1016/j.ijcard.2018.05.057. Epub 2018 Jun 2. Int J Cardiol. 2018. PMID: 30007487
-
High-risk plaque features can be detected in non-stenotic carotid plaques of patients with ischaemic stroke classified as cryptogenic using combined (18)F-FDG PET/MR imaging.Eur J Nucl Med Mol Imaging. 2016 Feb;43(2):270-279. doi: 10.1007/s00259-015-3201-8. Epub 2015 Oct 3. Eur J Nucl Med Mol Imaging. 2016. PMID: 26433367
-
Evaluation of ultrasmall superparamagnetic iron-oxide (USPIO) enhanced MRI with ferumoxytol to quantify arterial wall inflammation.Atherosclerosis. 2017 Aug;263:211-218. doi: 10.1016/j.atherosclerosis.2017.06.020. Epub 2017 Jun 8. Atherosclerosis. 2017. PMID: 28662398
-
Variability and uncertainty of 18F-FDG PET imaging protocols for assessing inflammation in atherosclerosis: suggestions for improvement.J Nucl Med. 2015 Apr;56(4):552-9. doi: 10.2967/jnumed.114.142596. Epub 2015 Feb 26. J Nucl Med. 2015. PMID: 25722452 Review.
-
Contemporary carotid imaging: from degree of stenosis to plaque vulnerability.J Neurosurg. 2016 Jan;124(1):27-42. doi: 10.3171/2015.1.JNS142452. Epub 2015 Jul 31. J Neurosurg. 2016. PMID: 26230478 Review.
Cited by
-
Multiparametric Imaging of Organ System Interfaces.Circ Cardiovasc Imaging. 2017 Apr;10(4):e005613. doi: 10.1161/CIRCIMAGING.116.005613. Circ Cardiovasc Imaging. 2017. PMID: 28360260 Free PMC article. Review.
-
18F-FDG Uptake on PET/CT in Symptomatic versus Asymptomatic Carotid Disease: a Meta-Analysis.Eur J Vasc Endovasc Surg. 2018 Aug;56(2):172-179. doi: 10.1016/j.ejvs.2018.03.028. Epub 2018 May 2. Eur J Vasc Endovasc Surg. 2018. PMID: 29730127 Free PMC article.
-
Molecular Imaging of Angiogenesis in Cardiac Regeneration.Curr Cardiovasc Imaging Rep. 2016;9(10):27. doi: 10.1007/s12410-016-9389-6. Epub 2016 Sep 10. Curr Cardiovasc Imaging Rep. 2016. PMID: 27683600 Free PMC article. Review.
-
Integrated cardiovascular assessment of atherosclerosis using PET/MRI.Br J Radiol. 2020 Sep 1;93(1113):20190921. doi: 10.1259/bjr.20190921. Epub 2020 Apr 3. Br J Radiol. 2020. PMID: 32238077 Free PMC article. Review.
-
18F-NaF PET/MRI for Detection of Carotid Atheroma in Acute Neurovascular Syndrome.Radiology. 2022 Oct;305(1):137-148. doi: 10.1148/radiol.212283. Epub 2022 Jun 7. Radiology. 2022. PMID: 35670715 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
