

Measuring Pediatric Bronchoscopy Outcomes Using an Electronic Medical Record
- PMID: 26816220
- PMCID: PMC6137899
- DOI: 10.1513/AnnalsATS.201509-576OC
Measuring Pediatric Bronchoscopy Outcomes Using an Electronic Medical Record
Abstract
Rationale: Bronchoscopy procedures should be tracked for safety, quality improvement, and federal regulations.
Objective: The aim of this study was to develop and test a method for evaluating flexible bronchoscopy use and outcomes using the electronic medical record (EMR) system in current clinical use at a large children's hospital.
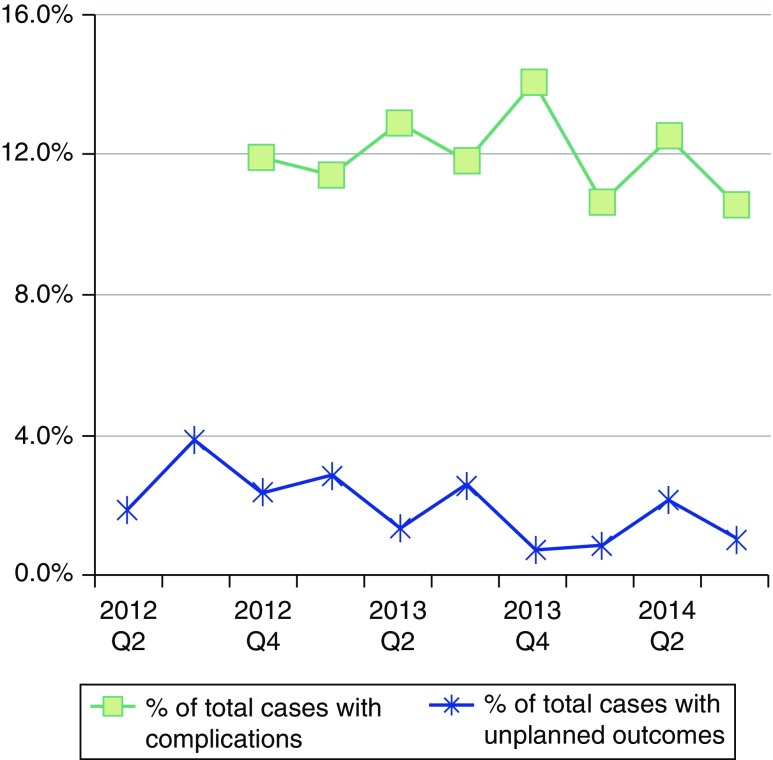
Methods: We created a custom bronchoscopy procedure note for our EMR system (Epic Systems Corporation) to track demographics, bronchoscopist, coordinated procedures, and outcome. Unplanned outcomes in children were defined as a disposition (admission to the hospital or elevation of care) after flexible bronchoscopy that differed from the preoperative plan. Readmissions to the hospital and emergency visits within our hospital system were also tracked electronically. Unplanned outcomes and readmissions were evaluated by a bronchoscopy quality team.
Measurements and main results: Over 2.5 years, we tracked 1,297 bronchoscopic procedures performed on 1,161 patients (60% male, 78% American Society of Anesthesiologists class 2 or 3, mean age 5.5 yr [range, 0.02-40 yr]). Overall, 27 unplanned outcomes occurred (2.1%). The risk of unplanned outcomes did not appear to be different between procedures performed by a trainee with faculty oversight and those performed by a faculty member alone. Patients with multiple same-day procedures were more likely to have unplanned outcomes (21 of 27 [78%], P = 0.004) than were patients who had flexible bronchoscopy alone. The relative risk (RR) of having an unplanned outcome was not different from flexible bronchoscopy alone in the subset of patients with multiple procedures coordinated through our multidisciplinary aerodigestive clinic (RR 0.7; 95% CI, 0.1-3.4). The risk of unplanned events was significantly elevated in children with coordinated procedures scheduled outside the aerodigestive group (RR, 5.8; 95% CI, 2.4-14.5). Ten patients (<1%) were readmitted or seen urgently within 1 week; three of these unplanned outcomes were attributed to complications of the bronchoscopy.
Conclusions: An EMR system may be used to track procedural outcomes. Unplanned outcomes after flexible bronchoscopy were infrequent at our institution. Children who underwent multiple procedures had unplanned outcomes more often; however, the subset of children who underwent coordinated procedures through our multidisciplinary aerodigestive clinic did not demonstrate this increased risk.
Keywords: aerodigestive; diagnostic techniques; flexible bronchoscopy; safety.
Figures
References
-
- Wood RE, Fink RJ. Applications of flexible fiberoptic bronchoscopes in infants and children. Chest. 1978;73:737–740. - PubMed
-
- Nussbaum E. Flexible fiberoptic bronchoscopy and laryngoscopy in children under 2 years of age: diagnostic and therapeutic applications of a new pediatric flexible fiberoptic bronchoscope. Crit Care Med. 1982;10:770–772. - PubMed
-
- Wood RE, Postma D. Endoscopy of the airway in infants and children. J Pediatr. 1988;112:1–6. - PubMed
-
- Fan LL, Sparks LM, Fix FJ. Flexible fiberoptic endoscopy for airway problems in a pediatric intensive care unit. Chest. 1988;93:556–560. - PubMed
-
- Stillwell PC, Radford PJ. Should all children with stridor undergo flexible bronchoscopy? J Bronchol. 1994;1:276–280.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
