

Multidisciplinary approach to non-surgical management of inguinal disruption in a professional hockey player treated with platelet-rich plasma, manual therapy and exercise: a case report
- PMID: 26816415
- PMCID: PMC4711326
Multidisciplinary approach to non-surgical management of inguinal disruption in a professional hockey player treated with platelet-rich plasma, manual therapy and exercise: a case report
Abstract
Objective: To present the clinical management of inguinal disruption in a professional hockey player and highlight the importance of a multidisciplinary approach to diagnosis and management.
Clinical features: A professional hockey player with recurrent groin pain presented to the clinic after an acute exacerbation of pain while playing hockey.
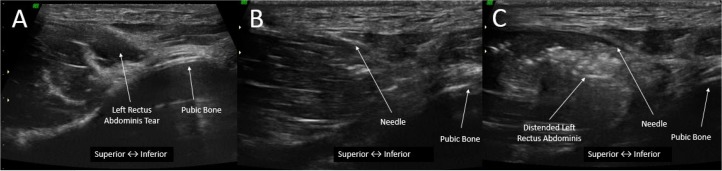
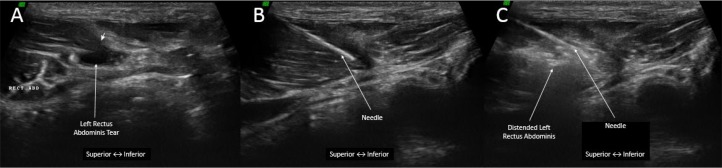
Intervention: The patient received a clinical diagnosis of inguinal disruption. Imaging revealed a tear in the rectus abdominis. Management included two platelet-rich plasma (PRP) injections to the injured tissue, and subsequent manual therapy and exercise. The patient returned to his prior level of performance in 3.5 weeks.
Discussion: This case demonstrated the importance of a multidisciplinary team and the need for advanced imaging in athletes with groin pain.
Summary: Research quality concerning the non-surgical management of inguinal disruption remains low. This case adds evidence that PRP, with the addition of manual therapy and exercise may serve as a relatively quick and effective non-surgical management strategy.
Objectif: Présenter la prise en charge clinique d’une perturbation inguinale chez un joueur de hockey et mettre en évidence l’importance que revêt une approche multidisciplinaire pour le diagnostic et la prise en charge.
Caractéristiques cliniques: Un joueur de hockey professionnel souffrant d’une douleur récurrente au niveau de l’aine s’est présenté à la clinique à la suite d’une exacerbation aiguë de la douleur survenue au cours de la pratique de son sport.
Intervention: Le patient a reçu un diagnostic clinique d’une perturbation inguinale. L’imagerie médicale a révélé la présence d’une déchirure au niveau du grand droit de l’abdomen. La prise en charge comprenait deux injections de plasma riche en plaquettes (PRP) dans le tissu lésé, ainsi qu’une thérapeutique manuelle et des exercices ultérieurs. Le patient a retrouvé son niveau de performance antérieur en 3,5 semaines.
Discussion: Ce cas prouve l’importance de recourir à une équipe pluridisciplinaire et la nécessité d’utiliser des technologies d’imagerie de pointe chez les athlètes souffrant de douleurs récurrentes au niveau de l’aine.
Résumé: La qualité des recherches relatives à la prise en charge non-chirurgicale des perturbations inguinales demeure faible. Ce cas est une preuve supplémentaire que le PRP, associé à une thérapeutique manuelle et à des exercices, peut constituer une stratégie de prise en charge non-chirurgicale relativement rapide et efficace.
Keywords: PRP; athletic pubalgia; chiropractic; inguinal disruption; platelet-rich plasma; sports hernia.
Figures







Similar articles
-
Athletic pubalgia and associated rehabilitation.Int J Sports Phys Ther. 2014 Nov;9(6):774-84. Int J Sports Phys Ther. 2014. PMID: 25383246 Free PMC article.
-
Proposed algorithm for the management of athletes with athletic pubalgia (sports hernia): a case series.J Orthop Sports Phys Ther. 2008 Dec;38(12):768-81. doi: 10.2519/jospt.2008.2846. J Orthop Sports Phys Ther. 2008. PMID: 19047766
-
Groin Injuries (Athletic Pubalgia) and Return to Play.Sports Health. 2016 Jul;8(4):313-23. doi: 10.1177/1941738116653711. Epub 2016 Jun 14. Sports Health. 2016. PMID: 27302153 Free PMC article. Review.
-
Nonsurgical Management of Adductor-related groin pain with Ultrasound-Guided Platelet-Rich Plasma Injection and Physical Therapy in a Competitive Soccer Player: A Case Report.Int J Sports Phys Ther. 2024 Jul 1;19(7):898-909. doi: 10.26603/001c.120209. eCollection 2024. Int J Sports Phys Ther. 2024. PMID: 38966832 Free PMC article.
-
Sports Hernias: A Comprehensive Review for Clinicians.Cureus. 2023 Aug 10;15(8):e43283. doi: 10.7759/cureus.43283. eCollection 2023 Aug. Cureus. 2023. PMID: 37692688 Free PMC article. Review.
Cited by
-
Total extraperitoneal laparoscopic inguinal hernia repair with adductor tenotomy: a 10-year experience in the treatment of athletic pubalgia.Surg Endosc. 2021 Jun;35(6):2743-2749. doi: 10.1007/s00464-020-07705-2. Epub 2020 Jun 16. Surg Endosc. 2021. PMID: 32556756
-
Sports hernia repair with adductor tenotomy.Hernia. 2017 Feb;21(1):139-147. doi: 10.1007/s10029-016-1520-8. Epub 2016 Aug 6. Hernia. 2017. PMID: 27497946
-
Effectiveness of Active Rehabilitation Program on Sports Hernia: Randomized Control Trial.Ann Rehabil Med. 2019 Jun;43(3):305-313. doi: 10.5535/arm.2019.43.3.305. Epub 2019 Jun 28. Ann Rehabil Med. 2019. PMID: 31311252 Free PMC article.
-
Chiropractic case reports: a review and bibliometric analysis.Chiropr Man Therap. 2021 Apr 28;29(1):17. doi: 10.1186/s12998-021-00374-5. Chiropr Man Therap. 2021. PMID: 33910610 Free PMC article. Review.
-
Investigating the research capacity and productivity of Canadian sports chiropractors.J Can Chiropr Assoc. 2023 Dec;67(3):202-225. J Can Chiropr Assoc. 2023. PMID: 38283160 Free PMC article.
References
-
- Caudill P, Nyland J, Smith C, Yerasimides J, Lach J. Sports hernias: a systematic literature review. Br J Sports Med. 2008;42(12):954–964. - PubMed
-
- Swan KG, Wolcott M. The athletic hernia: a systematic review. Clin Orthop Relat Res. 2007;455:78–87. - PubMed
-
- Yuill EA, Pajaczkowski JA, Howitt SD. Conservative care of sports hernias within soccer players: a case series. J Bodyw Mov Ther. 2012;16(4):540–548. - PubMed
-
- Campanelli G. Pubic inguinal pain syndrome: the so-called sports hernia. Hernia. 2010;14(1):1–4. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials