

Incidence and risk factors for food hypersensitivity in UK infants: results from a birth cohort study
- PMID: 26816616
- PMCID: PMC4727377
- DOI: 10.1186/s13601-016-0089-8
Incidence and risk factors for food hypersensitivity in UK infants: results from a birth cohort study
Abstract
Background: The prevalence of food hypersensitivity in the UK is still largely open to debate. Additionally its pathogenesis is also unclear although it is known that there are differing phenotypes. Determining its prevalence, along with identifying those factors associated with its development will help to assess its clinical importance within the national setting and also add to the debate on appropriate prevention strategies.
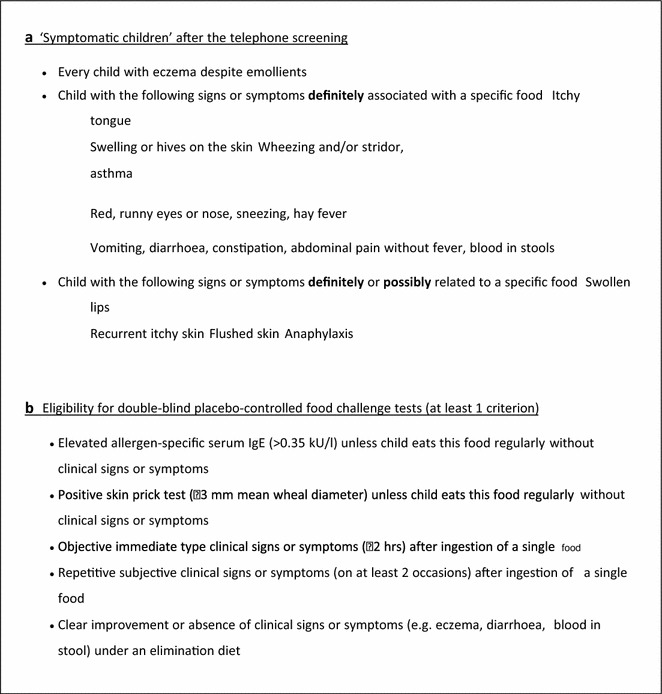
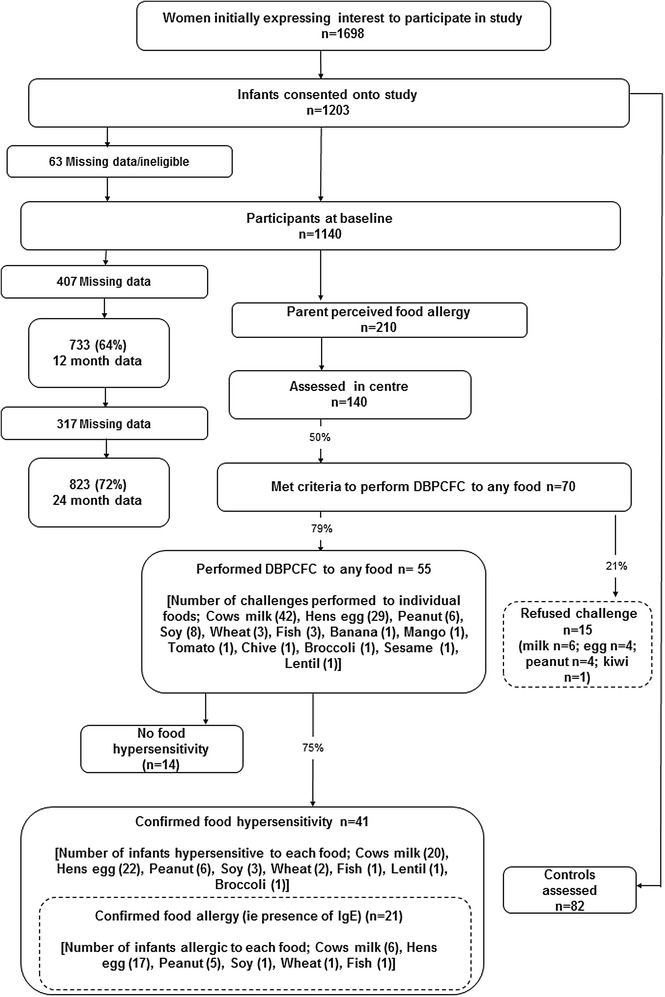
Methods: A population based birth cohort study conducted in Hampshire, UK as part of the EuroPrevall birth cohort study. 1140 infants were recruited with 823 being followed up until 2 years of age. Infants with suspected food reactions were assessed including specific IgE measurement and skin prick testing. Diagnosis of food hypersensitivity was by positive double-blind, placebo-controlled food challenge (DBPCFC) where symptoms up to 48 h after the end of the food challenge were considered indicative of a food hypersensitivity. Factors associated with food hypersensitivity and its two phenotypes of IgE-mediated and non-IgE-mediated disease were modelled in a multivariable logistic regression analysis.
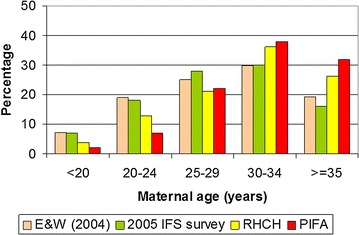
Results: Cumulative incidence of food hypersensitivity by 2 years of age was 5.0 %. The cumulative incidence for individual food allergens were hens' egg 2.7 % (1.6-3.8); cows' milk 2.4 % (1.4-3.5); peanut 0.7 % (0.1-1.3); soy 0.4 % (0.0-0.8); wheat 0.2 % (0.0-0.5) and 0.1 % (0.0-0.32) for fish. The cumulative incidence of IgE-mediated food allergy was 2.6 % with 2.1 % reacting to hens' egg. For non-IgE-mediated food allergy the cumulative incidence was 2.4 % (cows' milk 1.7 %). Predictors for any food hypersensitivity were wheeze, maternal atopy, increasing gestational age, age at first solid food introduction and mean healthy dietary pattern score. Predictors for IgE mediated allergy were eczema, rhinitis and healthy dietary pattern score whereas for non-IgE-mediated food allergy the predictors were dog in the home, healthy dietary pattern score, maternal consumption of probiotics during breastfeeding and age at first solid food introduction.
Conclusions: Just under half the infants with confirmed food hypersensitivity had no demonstrable IgE. In an exploratory analysis, risk factors for this phenotype of food hypersensitivity differed from those for IgE-mediated food allergy except for a healthy infant diet which was associated with less risk for both phenotypes.
Keywords: Dietary pattern analysis; Epidemiology; EuroPrevall; Food allergy; Food hypersensitivity; Healthy eating; Incidence; Risk factors.
Figures
References
-
- Voordouw J, Fox M, Cornelisse J, Antonides G, Mugford M, Frewer L. Household costs associated with food allergy: an exploratory study. British Food Journal. 2010;112(11):1205–1215. doi: 10.1108/00070701011088197. - DOI
-
- Nwaru BI, Hickstein L, Panesar SS, Muraro A, Werfel T, Cardona V, et al. The epidemiology of food allergy in Europe: a systematic review and meta-analysis. Allergy. 2014 (in press). - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
