

Management of the devastated posterior urethra and bladder neck: refractory incontinence and stenosis
- PMID: 26816811
- PMCID: PMC4708273
- DOI: 10.3978/j.issn.2223-4683.2015.02.02
Management of the devastated posterior urethra and bladder neck: refractory incontinence and stenosis
Abstract
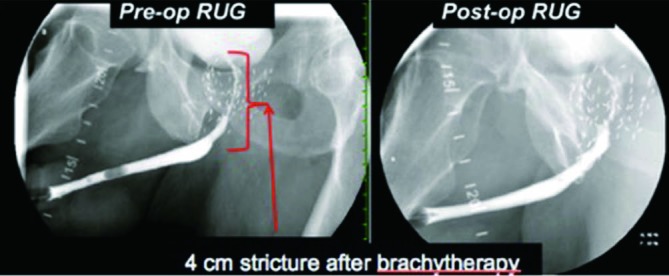
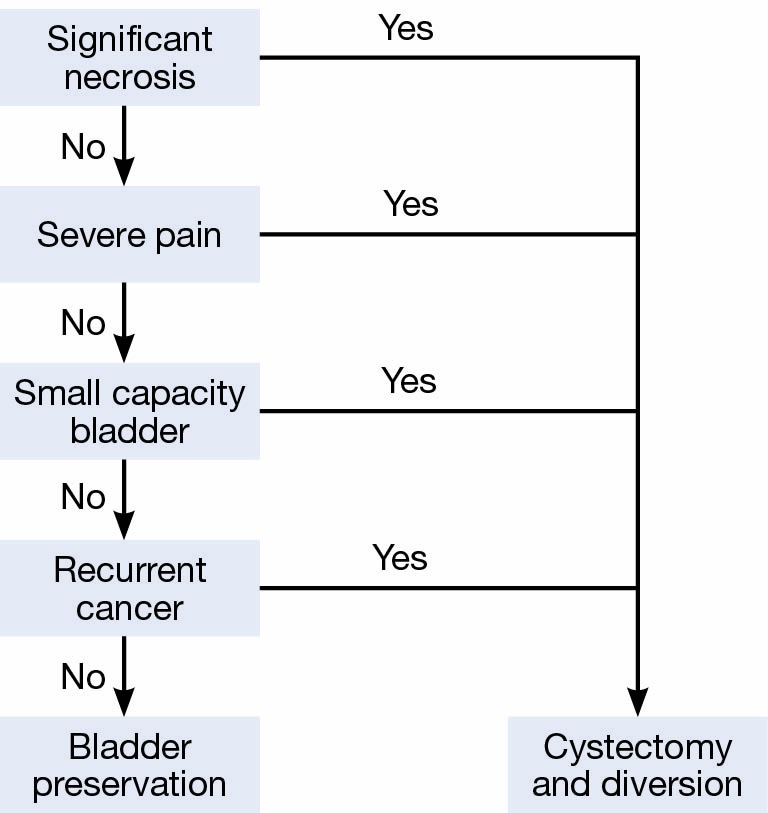
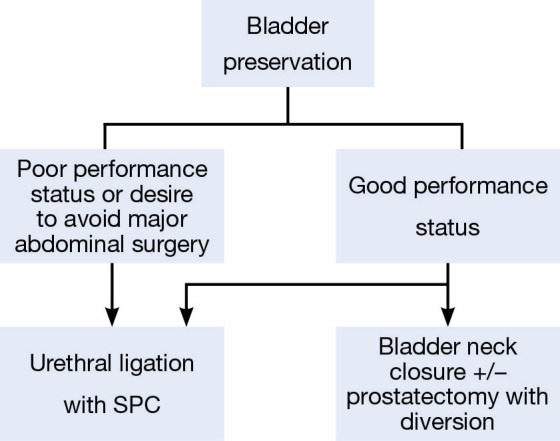
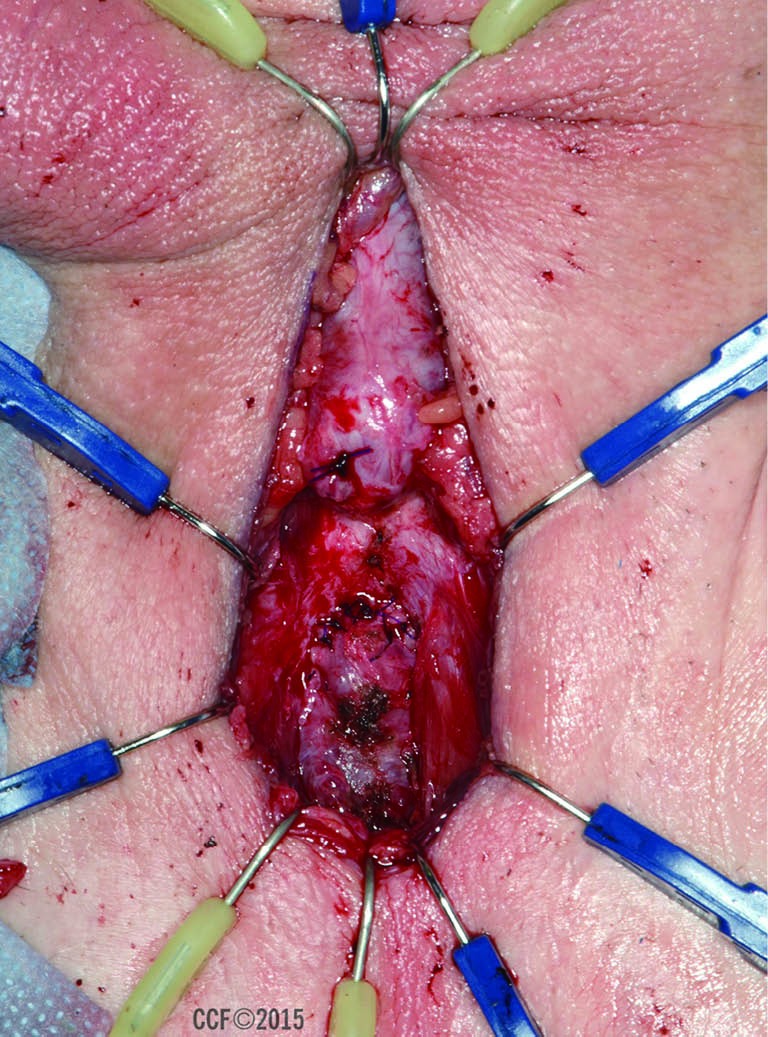
Stricture of the proximal urethra following treatment for prostate cancer occurs in an estimated 1-8% of patients. Following prostatectomy, urethral reconstruction is feasible in many patients. However, in those patients with prior radiation therapy (RT), failed reconstruction, refractory incontinence or multiple comorbidities, reconstruction may not be feasible. The purpose of this article is to review the evaluation and management options for patients who are not candidates for reconstruction of the posterior urethra and require urinary diversion. Patient evaluation should result in the decision whether reconstruction is feasible. In our experience, risk factors for failed reconstruction include prior radiation and multiple failed endoscopic treatments. Pre-operative cystoscopy is an essential part of the evaluations to identify tissue necrosis, dystrophic calcification, or tumor in the urethra, prostate and/or bladder. If urethral reconstruction is not feasible it is imperative to discuss options for urine diversion with the patient. Treatment options include simple catheter diversion, urethral ligation, and both bladder preserving and non-preserving diversion. Surgical management should address both the bladder and the bladder outlet. This can be accomplished from a perineal, abdominal or abdomino-perineal approach. The devastated bladder outlet is a challenging problem to treat. Typically, patients undergo multiple procedures in an attempt to restore urethral continuity and continence. For the small subset who fails reconstruction, urinary diversion provides a definitive, "end-stage" treatment resulting in improved quality of life.
Keywords: Bladder neck contracture (BNC); posterior urethral stenosis (PUS); prostate cancer; urethral stricture.
Conflict of interest statement
Figures

Similar articles
-
[Devastated bladder outlet-suprapubic catheter vs. reconstruction].Urologe A. 2020 Apr;59(4):408-415. doi: 10.1007/s00120-020-01153-5. Urologe A. 2020. PMID: 32125449 Review. German.
-
Devastated Bladder Outlet in Pelvic Cancer Survivors: Issues on Surgical Reconstruction and Quality of Life.J Clin Med. 2021 Oct 24;10(21):4920. doi: 10.3390/jcm10214920. J Clin Med. 2021. PMID: 34768438 Free PMC article. Review.
-
Management of the Devastated Bladder Outlet after Prostate CANCER Treatment.Curr Urol Rep. 2024 Jul;25(7):149-162. doi: 10.1007/s11934-024-01206-8. Epub 2024 May 16. Curr Urol Rep. 2024. PMID: 38750347 Review.
-
Management of Urethral Stricture and Bladder Neck Contracture Following Primary and Salvage Treatment of Prostate Cancer.Curr Urol Rep. 2017 Oct;18(10):76. doi: 10.1007/s11934-017-0729-0. Curr Urol Rep. 2017. PMID: 28776126 Review.
-
The devastated bladder outlet: treatment options.Curr Opin Urol. 2015 Jul;25(4):352-6. doi: 10.1097/MOU.0000000000000185. Curr Opin Urol. 2015. PMID: 26049880 Review.
Cited by
-
[Devastated bladder outlet-suprapubic catheter vs. reconstruction].Urologe A. 2020 Apr;59(4):408-415. doi: 10.1007/s00120-020-01153-5. Urologe A. 2020. PMID: 32125449 Review. German.
-
Transperineal reanastomosis for treatment of highly recurrent anastomotic strictures after radical retropubic prostatectomy: extended follow-up.World J Urol. 2017 Dec;35(12):1885-1890. doi: 10.1007/s00345-017-2067-8. Epub 2017 Jul 3. World J Urol. 2017. PMID: 28674908
-
Devastated Bladder Outlet in Pelvic Cancer Survivors: Issues on Surgical Reconstruction and Quality of Life.J Clin Med. 2021 Oct 24;10(21):4920. doi: 10.3390/jcm10214920. J Clin Med. 2021. PMID: 34768438 Free PMC article. Review.
-
Management of the Devastated Bladder Outlet after Prostate CANCER Treatment.Curr Urol Rep. 2024 Jul;25(7):149-162. doi: 10.1007/s11934-024-01206-8. Epub 2024 May 16. Curr Urol Rep. 2024. PMID: 38750347 Review.
-
[Bladder neck sclerosis following prostate surgery : Which therapy when?].Urologe A. 2017 Sep;56(9):1129-1138. doi: 10.1007/s00120-017-0431-3. Urologe A. 2017. PMID: 28646238 Review. German.
References
-
- Flynn BJ, Delvecchio FC, Webster GD. Perineal repair of pelvic fracture urethral distraction defects: experience in 120 patients during the last 10 years. J Urol 2003;170:1877-80. - PubMed
-
- Turner-Warwick R. Urethral stricture surgery. In: Mundy A. eds. Current operative surgery—urology. London: Bailliere Tindall, 1988:160-218.
-
- Morey AF, McAninch JW. Reconstruction of posterior urethral disruption injuries: outcome analysis in 82 patients. J Urol 1997;157:506-10. - PubMed
-
- Mundy AR, Andrich DE. Posterior urethral complications of the treatment of prostate cancer. BJU Int 2012;110:304-25. - PubMed
-
- Carr LK, Webster GD. Endoscopic management of the obliterated anastomosis following radical prostatectomy. J Urol 1996;156:70-2. - PubMed
Publication types
LinkOut - more resources
Full Text Sources