

Prevalence of Human Papillomavirus Genotypes Among Women With High-Grade Cervical Lesions in Beijing, China
- PMID: 26817906
- PMCID: PMC4998280
- DOI: 10.1097/MD.0000000000002555
Prevalence of Human Papillomavirus Genotypes Among Women With High-Grade Cervical Lesions in Beijing, China
Abstract
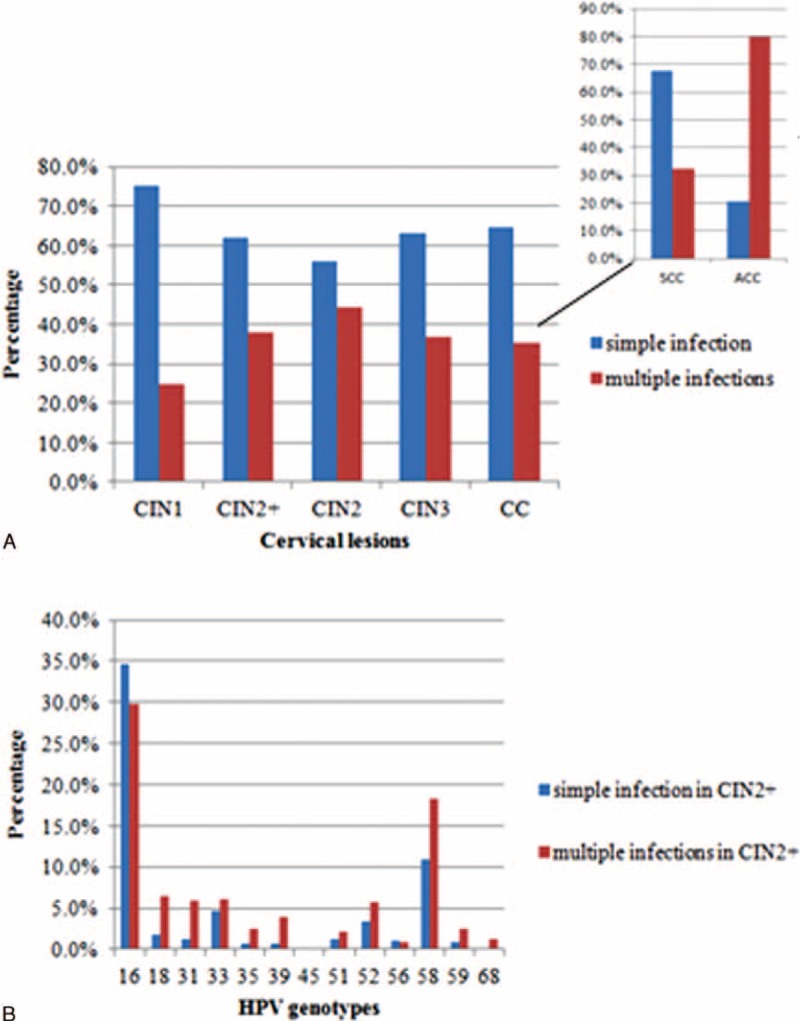
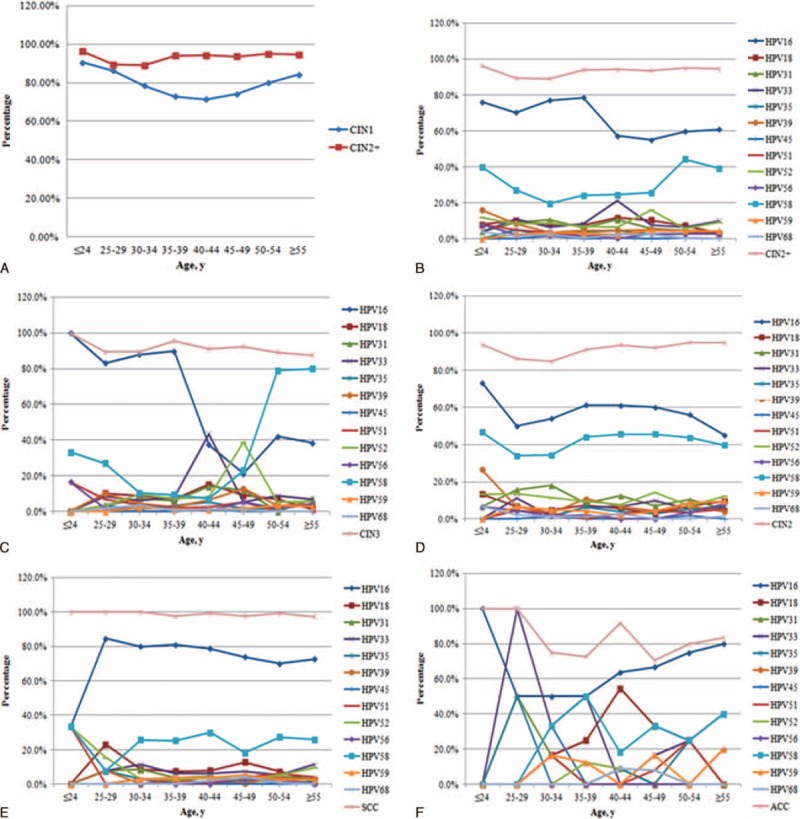
The aim of the study is to investigate the prevalence of high-risk human papillomavirus (hr-HPV) genotypes among Han women with high-grade cervical lesions in Beijing, China.Cervical cell specimens from patients with histopathologically confirmed cervical lesions at 7 hospitals in Beijing were examined with a validated HPV kit for 13 hr-HPV genotypes during the study period. The patients were divided into a low-grade cervical lesions group (cervical intraepithelial neoplasia grade 1, CIN1) and a high-grade cervical lesions group (CIN2+, including cervical intraepithelial neoplasia grade 2, CIN2; cervical intraepithelial neoplasia grade 3, CIN3; squamous cervical cancer, SCC; and adenocarcinoma of the cervix, ACC) based on the histopathology results.A total of 2817 eligible patients were enrolled, including 610 cases identified as CIN1 and 2207 as CIN2+. The hr-HPV positive rates in the CIN1 and CIN2+ groups were 78.2% (477/610) and 93.3% (2060/2207), respectively. The most frequently detected genotypes were HPV16, 58, 52 and18 in the CIN1 group and HPV16, 58, 33, and 52 in the CIN2+ group, in descending order of prevalence. In addition, the prevalence of HPV18 among the patients with ACC was 28.6% (14/49), significantly >7.2% (54/752) prevalence among the SCC patients (P < 0.001). Additionally, significantly more women in the CIN2+ group had multiple infections compared with those in the CIN1 group (38.1% and 24.9%, respectively; P < 0.001). However, as the cervical lesion grade increased, the prevalence of multiple hr-HPV infections gradually deceased to 44.2% in the CIN2 patients, 36.7% in the CIN3 patients, and 35.3% in the cervical cancer (CC) patients, which included SCC and ACC patients. In cases of multiple hr-HPV infections in the CIN2+ group, double infections accounted for ∼76.6%, and HPV16+58, HPV16+52, and HPV16+18 were the most common combinations, in descending order. The most frequent combination for triple infections was HPV16+58+31, with a rate of 4.2%. The highest positive rate occurred in the ≤24 year-old group for all types of cervical lesions.The prevalence of HPV genotypes in the targeted population with high-grade cervical lesions differs from that of other countries. This information could be helpful for the prevention of CC in Beijing, China.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures

Similar articles
-
Distribution of human papillomavirus genotypes in cervical intraepithelial neoplasia and invasive cervical cancer in Canada.J Med Virol. 2011 Jun;83(6):1034-41. doi: 10.1002/jmv.22081. J Med Virol. 2011. PMID: 21503917
-
High-risk human papillomavirus genotype distribution and attribution to cervical cancer and precancerous lesions in a rural Chinese population.J Gynecol Oncol. 2017 Jul;28(4):e30. doi: 10.3802/jgo.2017.28.e30. J Gynecol Oncol. 2017. PMID: 28541628 Free PMC article.
-
[Evaluation of CIN2+ /CIN3+ risk of different HPV subtypes infection combined with abnormal cytology status].Zhonghua Zhong Liu Za Zhi. 2018 Mar 23;40(3):232-238. doi: 10.3760/cma.j.issn.0253-3766.2018.03.015. Zhonghua Zhong Liu Za Zhi. 2018. PMID: 29575846 Chinese.
-
Prevalence and distribution of human papillomavirus genotypes in cervical intraepithelial neoplasia in China: a meta-analysis.Arch Gynecol Obstet. 2020 Dec;302(6):1329-1337. doi: 10.1007/s00404-020-05787-w. Epub 2020 Sep 10. Arch Gynecol Obstet. 2020. PMID: 32914222 Free PMC article. Review.
-
Impact of human papillomavirus types on uterine cervical neoplasia.J Obstet Gynaecol Res. 2024 Aug;50(8):1283-1288. doi: 10.1111/jog.15995. Epub 2024 Jun 9. J Obstet Gynaecol Res. 2024. PMID: 38852606 Review.
Cited by
-
Current Updates on Cancer-Causing Types of Human Papillomaviruses (HPVs) in East, Southeast, and South Asia.Cancers (Basel). 2021 May 30;13(11):2691. doi: 10.3390/cancers13112691. Cancers (Basel). 2021. PMID: 34070706 Free PMC article. Review.
-
Prevalence of human papillomavirus genotypes and relative risk of cervical cancer in China: a systematic review and meta-analysis.Oncotarget. 2018 Jan 11;9(20):15386-15397. doi: 10.18632/oncotarget.24169. eCollection 2018 Mar 16. Oncotarget. 2018. PMID: 29632652 Free PMC article.
-
Relationship between Human Papillomavirus Prevalence and DNA Damage in Cervical Cancer Population in Gansu Province, China.Intervirology. 2022;65(4):215-223. doi: 10.1159/000525975. Epub 2022 Jul 12. Intervirology. 2022. PMID: 35820368 Free PMC article.
-
Analysis of HPV distribution in patients with cervical precancerous lesions in Western China.Medicine (Baltimore). 2017 Jul;96(29):e7304. doi: 10.1097/MD.0000000000007304. Medicine (Baltimore). 2017. PMID: 28723743 Free PMC article.
-
Human papillomavirus genotypes associated with cervical precancerous lesions and cancer in the highest area of cervical cancer mortality, Longnan, China.Infect Agent Cancer. 2017 Jan 25;12:8. doi: 10.1186/s13027-017-0116-y. eCollection 2017. Infect Agent Cancer. 2017. PMID: 28138337 Free PMC article.
References
-
- Lindsey AT, Freddie B, Rebecca LS, et al. Global cancer statistics, 2012. CA Cancer J Clin 2015; 65:87–108. - PubMed
-
- Bosch FX, Manos MM, Munoz N, et al. Prevalence of human papillomavirus in cervical cancer: a worldwide perspective. J Natl Cancer Inst 1995; 87:796–802. - PubMed
-
- Silvia de S, Wim GVQ, Laia A, et al. Human papillomavirus genotype attribution in invasive cervical cancer: a retrospective cross-sectional worldwide study. Lancet Oncol 2010; 11:1048–1056. - PubMed
-
- Thomas CW, Mark HS, Catherine MB, et al. The ATHENA human papillomavirus study: design, methods, and baseline results. Am J Obstet Gynecol 2012; 206:46.e1–11. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
