

Management of patients with issues related to opioid safety, efficacy and/or misuse: a case series from an integrated, interdisciplinary clinic
- PMID: 26818474
- PMCID: PMC4730605
- DOI: 10.1186/s13722-016-0050-0
Management of patients with issues related to opioid safety, efficacy and/or misuse: a case series from an integrated, interdisciplinary clinic
Abstract
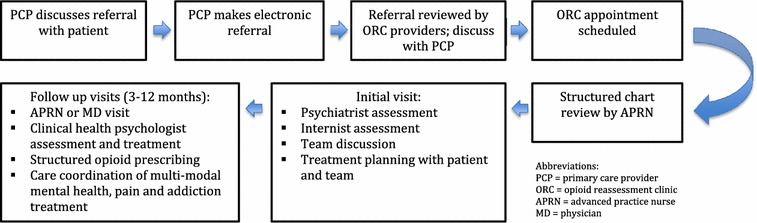
Background: Patients, providers, communities and health systems have struggled to achieve balance between access to opioid treatment for chronic pain and its potential harmful consequences: especially misuse, addiction and overdose. We developed an interdisciplinary clinic embedded within primary care (the Opioid Reassessment Clinic-ORC) with the goal of improving the quality of care of patients with co-occurring chronic pain and issues related to opioid safety, efficacy and/or misuse.
Case descriptions: We present three cases referred to the ORC that highlight complex clinical scenarios related to assessment and treatment of patients with chronic pain and issues related to opioid safety, efficacy and misuse.
Discussion and evaluation: In the context of the three cases, with respect to assessment, we discuss: making the diagnosis of opioid use disorder; allowing the patient space to endorse lack of efficacy; identification of co-occurring hazardous alcohol use; and recognizing barriers to multimodal pain care. With respect to treatment, we discuss: making a change in treatment with which the patient may not agree; effectiveness of buprenorphine/naloxone for the treatment of chronic pain; responding to low efficacy; and making continued opioid therapy contingent on engagement with substance abuse treatment.
Conclusions: The core components of our approach-biopsychosocial assessment and multimodal treatment planning with an emphasis on promoting functional goals and safety using clear communication and a patient-centered stance-should guide providers in the management of similar clinical scenarios. More evidence is needed to definitively guide specific interventions and points of clinical equipoise.
References
-
- Centers for Disease Control and Prevention . Policy impact: prescription painkiller overdoses. Atlanta: Centers for Disease Control and Prevention; 2011.
-
- The Management for Opioid Therapy for Chronic Pain Working Group . VA/DoD clinical practice guideline for management of opioid therapy for chronic pain. 2. Washington: Department of Veterans Affairs and Department of Defense, Office of Quality and Performance; 2010.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
