

Myofibroblast secretome and its auto-/paracrine signaling
- PMID: 26818589
- PMCID: PMC4932866
- DOI: 10.1586/14779072.2016.1147348
Myofibroblast secretome and its auto-/paracrine signaling
Abstract
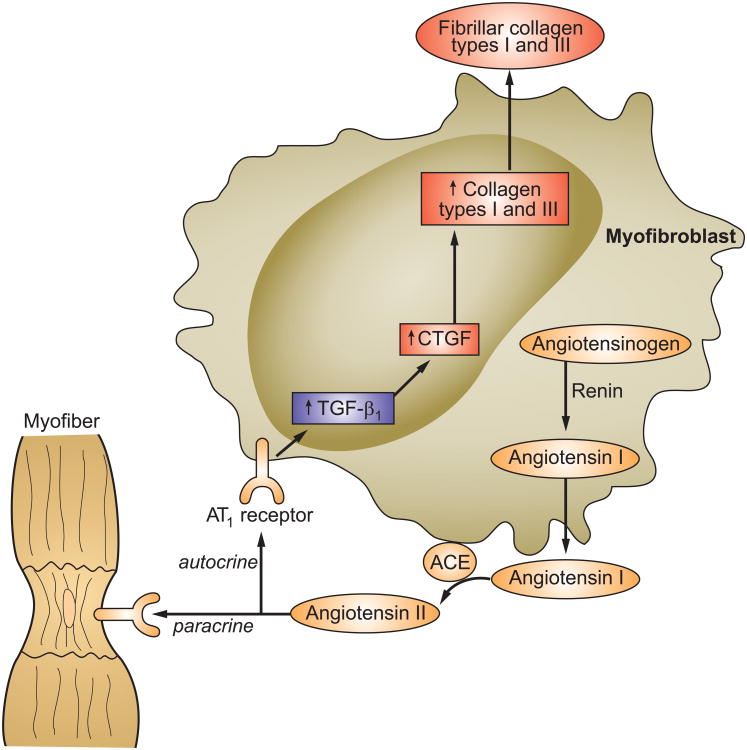
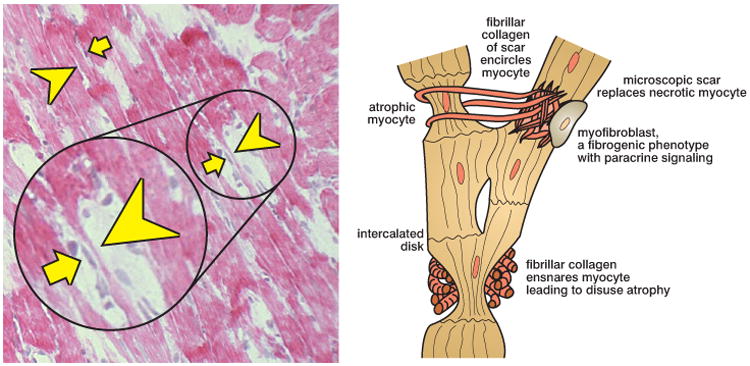
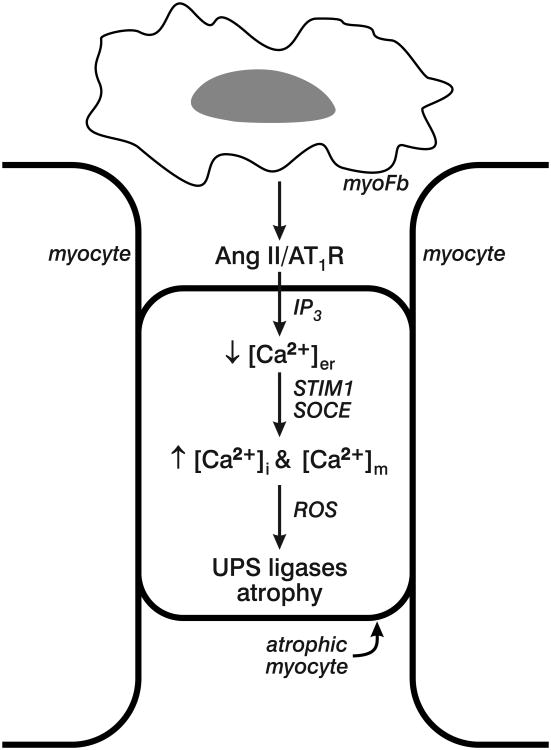
Myofibroblasts (myoFb) are phenotypically transformed, contractile fibroblast-like cells expressing α-smooth muscle actin microfilaments. They are integral to collagen fibrillogenesis with scar tissue formation at sites of repair irrespective of the etiologic origins of injury or tissue involved. MyoFb can persist long after healing is complete, where their ongoing turnover of collagen accounts for a progressive structural remodeling of an organ (a.k.a. fibrosis, sclerosis or cirrhosis). Such persistent metabolic activity is derived from a secretome consisting of requisite components in the de novo generation of angiotensin (Ang) II. Autocrine and paracrine signaling induced by tissue AngII is expressed via AT1 receptor ligand binding to respectively promote: i) regulation of myoFb collagen synthesis via the fibrogenic cytokine TGF-β1-Smad pathway; and ii) dedifferentiation and protein degradation of atrophic myocytes immobilized and ensnared by fibrillar collagen at sites of scarring. Several cardioprotective strategies in the prevention of fibrosis and involving myofibroblasts are considered. They include: inducing myoFb apoptosis through inactivation of antiapoptotic proteins; AT1 receptor antagonist to interfere with auto-/paracrine myoFb signaling or to induce counterregulatory expression of ACE2; and attacking the AngII-AT1R-TGF-β1-Smad pathway by antibody or the use of triplex-forming oligonucleotides.
Keywords: Cardiac fibrosis; angiotensin II; auto-/paracrine signaling; cardioprotection; myofibroblast secretome.
Figures
References
-
- Cotran RS, Kumar V, Robbins SL. The heart. In: Cotran RS, Kumar V, Robbins SL, editors. Robbins Pathologic Basis of Disease. 4th. Philadelphia: W B Saunders; 1989. pp. 597–656.
-
- Pearlman ES, Weber KT, Janicki JS, Pietra GG, Fishman AP. Muscle fiber orientation and connective tissue content in the hypertrophied human heart. Lab Invest. 1982;46:158–164. - PubMed
-
- Beltrami CA, Finato N, Rocco M, et al. Structural basis of end-stage failure in ischemic cardiomyopathy in humans. Circulation. 1994;89:151–163. **The presence of widely scattered foci of fibrosis found in the explanted failing human heart of ischemic origins. - PubMed
-
- Factor SM, Butany J, Sole MJ, et al. Pathologic fibrosis and matrix connective tissue in the subaortic myocardium of patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 1991;17:1343–1351. - PubMed
-
- Choudhury L, Mahrholdt H, Wagner A, et al. Myocardial scarring in asymptomatic or mildly symptomatic patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 2002;40:2156–2164. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous