

Strategies to estimate the characteristics of 24-hour IOP curves of treated glaucoma patients during office hours
- PMID: 26818941
- PMCID: PMC4728814
- DOI: 10.1186/s12886-016-0191-7
Strategies to estimate the characteristics of 24-hour IOP curves of treated glaucoma patients during office hours
Abstract
Background: It is known that office-hour measurements might not adequately estimate IOP mean, peaks and fluctuations in healthy subjects. The purpose of the present study is to verify whether office-hour measurements in patients in different body positions can estimate the characteristics of 24-hour intraocular pressure (IOP) in treated POAG patients.
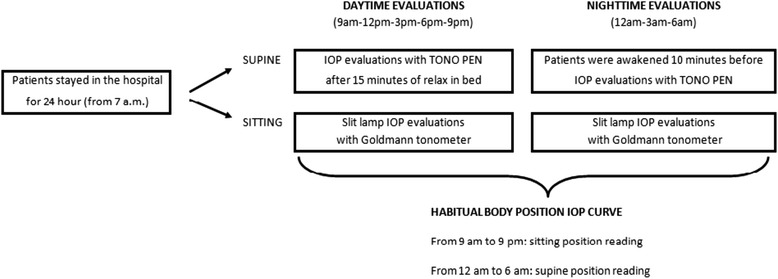
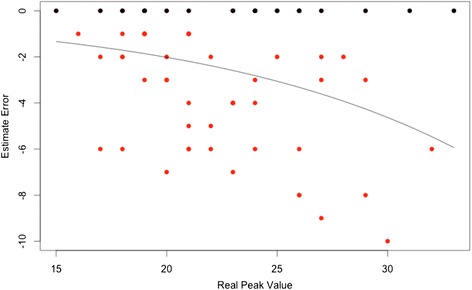
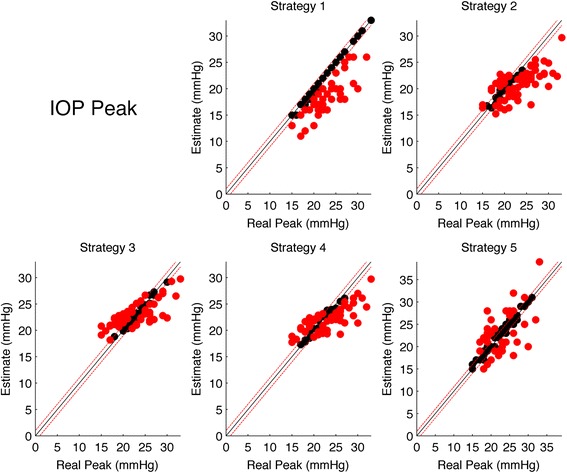
Methods: The 24-hour IOP curves of 70 eyes of 70 caucasian patients with treated glaucoma were analyzed. Measurements were taken at 9 AM; 12, 3, 6, and 9 PM; and 12, 3, and 6 AM, both in the supine (TonoPen XL) and sitting (Goldmann tonometer) positions. The ability of five strategies to estimate IOP mean, peak and fluctuation was evaluated. Each method was analyzed both with regression of the estimate error on the real value and with "hit or miss" analysis.
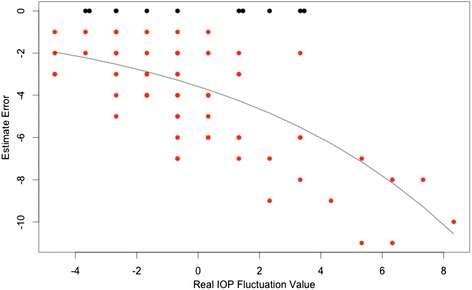
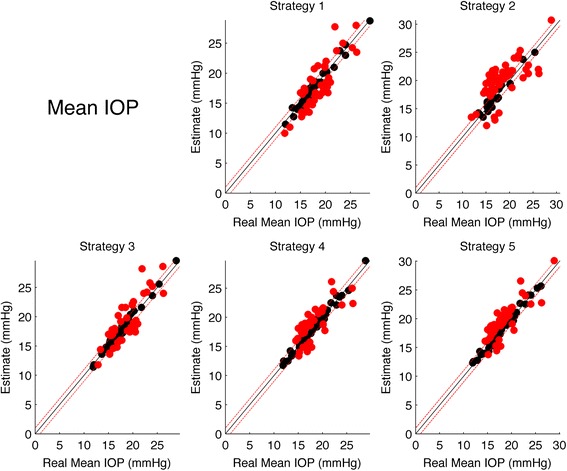
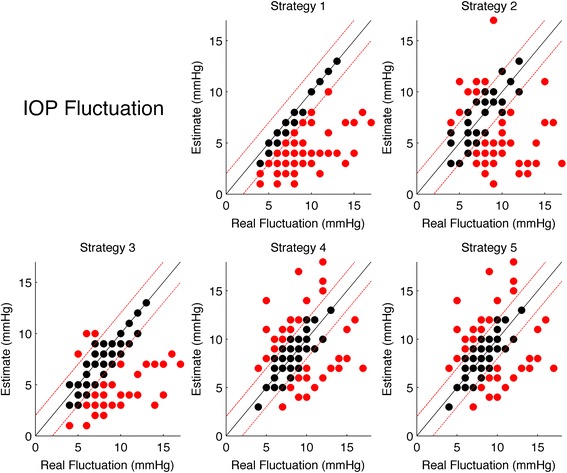
Results: The least biased estimate of the Peak IOP was obtained using measurements from both supine and sitting positions, also yielding the highest rate of correct predictions (which was significantly different from 3 of the remaining 4 strategies proposed, p < 0.05). Strategies obtained from the combination of supine, sitting and peak measurements resulted to be least biased for the Mean IOP and the IOP Fluctuation estimate, but all strategies were not found significantly different in terms of correct prediction rate (the only significant difference being between the two strategies based on sitting or supine measurements only, with the former being the one with the highest correct prediction rate).
Conclusions: The results of this study remark the concept that IOP is a dynamic parameter and that intensive measurement is helpful in determining its characteristics. All office-hour strategies showed a very poor performance of in correctly predicting the considered parameters within the thresholds used in this paper, all scoring a correct prediction rate below 52%.
Figures
References
-
- Lichter PR, Musch DC, Gillespie BW, Guire KE, Janz NK, Wren PA, et al. Interim clinical outcomes in the Collaborative Initial Glaucoma Treatment Study comparing initial treatment randomized to medications or surgery. Ophthalmology. 2001;108:1943–53. doi: 10.1016/S0161-6420(01)00873-9. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
