

Heart failure outcomes with empagliflozin in patients with type 2 diabetes at high cardiovascular risk: results of the EMPA-REG OUTCOME® trial
- PMID: 26819227
- PMCID: PMC4872285
- DOI: 10.1093/eurheartj/ehv728
Heart failure outcomes with empagliflozin in patients with type 2 diabetes at high cardiovascular risk: results of the EMPA-REG OUTCOME® trial
Abstract
Aims: We previously reported that in the EMPA-REG OUTCOME(®) trial, empagliflozin added to standard of care reduced the risk of 3-point major adverse cardiovascular events, cardiovascular and all-cause death, and hospitalization for heart failure in patients with type 2 diabetes and high cardiovascular risk. We have now further investigated heart failure outcomes in all patients and in subgroups, including patients with or without baseline heart failure.
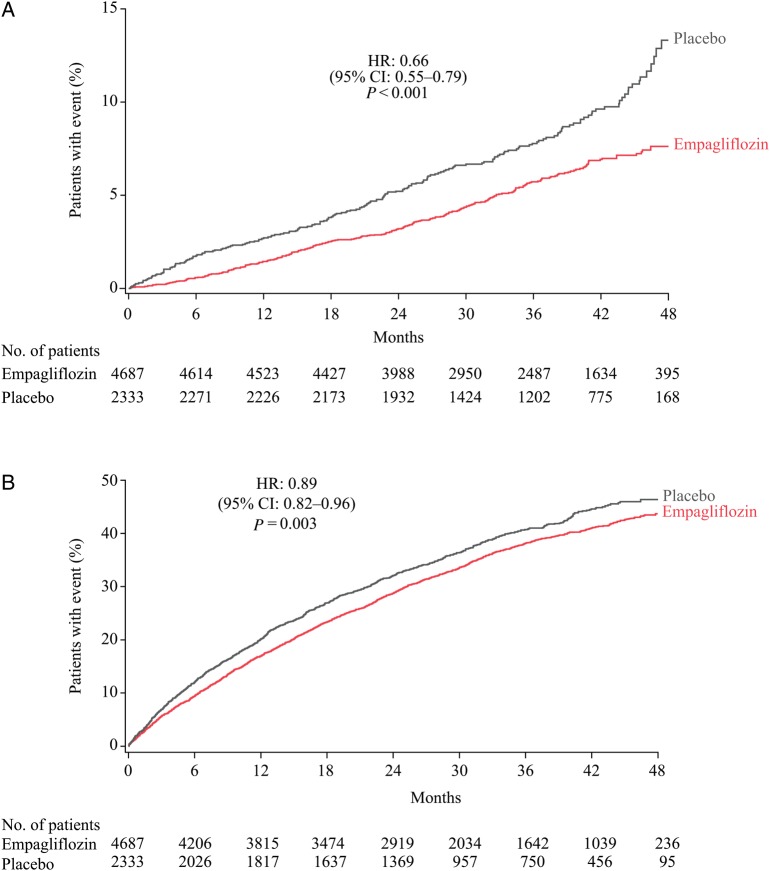
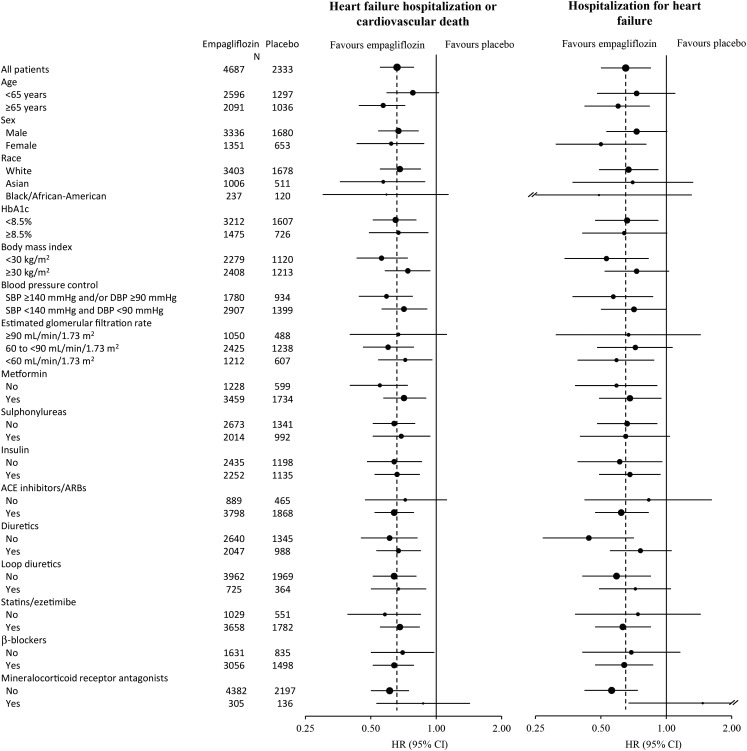
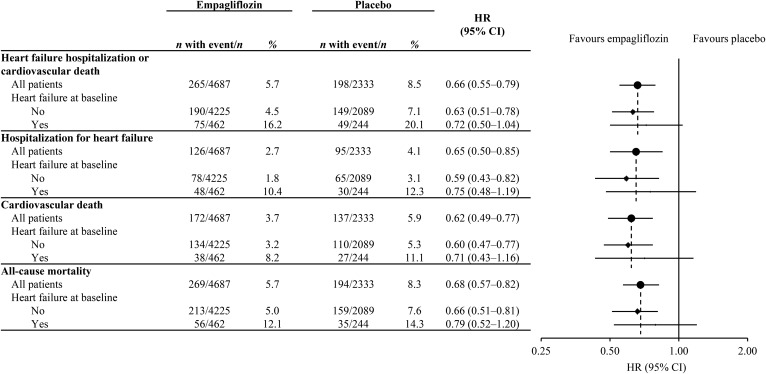
Methods and results: Patients were randomized to receive empagliflozin 10 mg, empagliflozin 25 mg, or placebo. Seven thousand and twenty patients were treated; 706 (10.1%) had heart failure at baseline. Heart failure hospitalization or cardiovascular death occurred in a significantly lower percentage of patients treated with empagliflozin [265/4687 patients (5.7%)] than with placebo [198/2333 patients (8.5%)] [hazard ratio, HR: 0.66 (95% confidence interval: 0.55-0.79); P < 0.001], corresponding to a number needed to treat to prevent one heart failure hospitalization or cardiovascular death of 35 over 3 years. Consistent effects of empagliflozin were observed across subgroups defined by baseline characteristics, including patients with vs. without heart failure, and across categories of medications to treat diabetes and/or heart failure. Empagliflozin improved other heart failure outcomes, including hospitalization for or death from heart failure [2.8 vs. 4.5%; HR: 0.61 (0.47-0.79); P < 0.001] and was associated with a reduction in all-cause hospitalization [36.8 vs. 39.6%; HR: 0.89 (0.82-0.96); P = 0.003]. Serious adverse events and adverse events leading to discontinuation were reported by a higher proportion of patients with vs. without heart failure at baseline in both treatment groups, but were no more common with empagliflozin than with placebo.
Conclusion: In patients with type 2 diabetes and high cardiovascular risk, empagliflozin reduced heart failure hospitalization and cardiovascular death, with a consistent benefit in patients with and without baseline heart failure.
Keywords: Cardiovascular disease; Hospitalization; Mortality.
© The Author 2016. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Erratum for
-
Treatment of diabetes and heart failure: joint forces.Eur Heart J. 2016 May 14;37(19):1535-7. doi: 10.1093/eurheartj/ehw039. Epub 2016 Feb 22. Eur Heart J. 2016. PMID: 26908942 No abstract available.
Comment in
-
Treatment of diabetes and heart failure: joint forces.Eur Heart J. 2016 May 14;37(19):1535-7. doi: 10.1093/eurheartj/ehw039. Epub 2016 Feb 22. Eur Heart J. 2016. PMID: 26908942 No abstract available.
-
Heart failure: SGLT2 inhibitors and heart failure -- clinical implications.Nat Rev Cardiol. 2016 Apr;13(4):185-6. doi: 10.1038/nrcardio.2016.35. Epub 2016 Mar 10. Nat Rev Cardiol. 2016. PMID: 26961066
References
-
- Bertoni AG, Hundley WG, Massing MW, Bonds DE, Burke GL, Goff DC Jr. Heart failure prevalence, incidence, and mortality in the elderly with diabetes. Diabetes Care 2004;27:699–703. - PubMed
-
- Cubbon RM, Adams B, Rajwani A, Mercer BN, Patel PA, Gherardi G, Gale CP, Batin PD, Ajjan R, Kearney L, Wheatcroft SB, Sapsford RJ, Witte KK, Kearney MT. Diabetes mellitus is associated with adverse prognosis in chronic heart failure of ischaemic and non-ischaemic aetiology. Diab Vasc Dis Res 2013;10:330–336. - PubMed
-
- Turnbull FM, Abraira C, Anderson RJ, Byington RP, Chalmers JP, Duckworth WC, Evans GW, Gerstein HC, Holman RR, Moritz TE, Neal BC, Ninomiya T, Patel AA, Paul SK, Travert F, Woodward M. Intensive glucose control and macrovascular outcomes in type 2 diabetes. Diabetologia 2009;52:2288–2298. - PubMed
-
- Lago RM, Singh PP, Nesto RW. Congestive heart failure and cardiovascular death in patients with prediabetes and type 2 diabetes given thiazolidinediones: a meta-analysis of randomised clinical trials. Lancet 2007;370:1129–1136. - PubMed
