

Hemostasis in liver transplantation: Pathophysiology, monitoring, and treatment
- PMID: 26819521
- PMCID: PMC4721987
- DOI: 10.3748/wjg.v22.i4.1541
Hemostasis in liver transplantation: Pathophysiology, monitoring, and treatment
Abstract
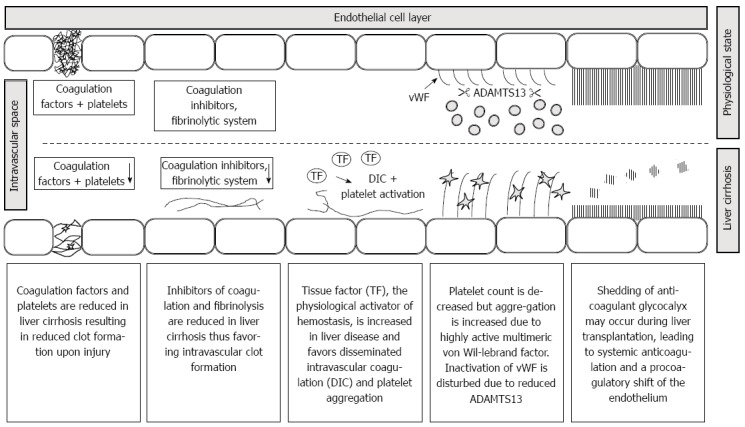
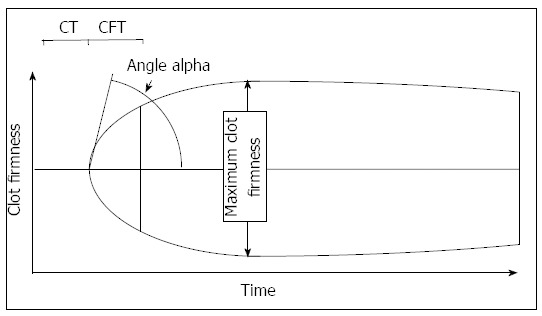
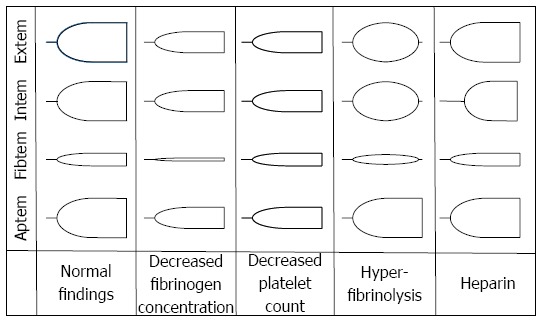
Recent findings in the pathophysiology and monitoring of hemostasis in patients with end stage liver disease have major impact on coagulation management during liver transplantation. There is increasing evidence, that the changes in both coagulation factors and platelet count regularly observed in patients with liver cirrhosis cannot be interpreted as a reliable indicator of diffuse bleeding risk. Instead, a differentiated view on hemostasis has led to the concept of a rebalanced coagulation system: While it is important to recognize that procoagulant factors are reduced in liver cirrhosis, it is also evident that synthesis of anticoagulant factors and fibrinolytic proteins produced in the liver is also diminished. Similarly, the decreased platelet count may be counterbalanced by increased platelet aggregability caused by highly active von Willebrand multimeres. The coagulation system is therefor stated to be rebalanced. While under normal "unstressed" conditions diffuse bleeding is rarely observed, however both diffuse bleeding or thrombus formation may occur when compensation mechanisms are exhausted. While most patients presenting for liver transplantation have severe cirrhosis, liver function and thus production of pro- and anticoagulant factors can be preserved especially in cholestatic liver disease. During liver transplantation, profound changes in the hemostasis system can occur. Surgical bleeding can lead to diffuse bleeding as coagulation factors and platelets are already reduced. Ischemia and tissue trauma can lead to alterations of hemostasis comparable to trauma induced coagulopathy. A further common disturbance often starting with the reperfusion of the transplanted organ is hyperfibrinolysis which can eventually precipitate complete consumption of fibrinogen and an endogenous heparinization by glycocalyx shedding. Moreover, thrombotic events in liver transplantations are not uncommon and contribute to increased mortality. Besides conventional laboratory methods, bed-side monitoring of hemostasis (e.g., thrombelastography, thrombelastometry) is often used during liver transplantation to rapidly diagnose decreases in fibrinogen and platelet count as well as hyperfibrinolysis and to guide treatment with blood products, factor concentrates, and antifibrinolytics. There is also evidence which suggests when algorithms based on bed-side hemostasis monitoring are used a reduction of blood loss, blood product use, and eventual mortality are possible. Notably, the bed-side monitoring of anticoagulant pathways and the thrombotic risk is not possible at time and thus a cautious and restrictive use of blood products is recommended.
Keywords: Bed-side monitoring; Coagulation factors; Hemostasis; Liver transplantation; Thrombelastography; Thrombelastometry.
Figures
References
-
- Kamath PS, Wiesner RH, Malinchoc M, Kremers W, Therneau TM, Kosberg CL, D’Amico G, Dickson ER, Kim WR. A model to predict survival in patients with end-stage liver disease. Hepatology. 2001;33:464–470. - PubMed
-
- Wada H, Usui M, Sakuragawa N. Hemostatic abnormalities and liver diseases. Semin Thromb Hemost. 2008;34:772–778. - PubMed
-
- Hugenholtz GC, Adelmeijer J, Meijers JC, Porte RJ, Stravitz RT, Lisman T. An unbalance between von Willebrand factor and ADAMTS13 in acute liver failure: implications for hemostasis and clinical outcome. Hepatology. 2013;58:752–761. - PubMed
-
- Lisman T, Bongers TN, Adelmeijer J, Janssen HL, de Maat MP, de Groot PG, Leebeek FW. Elevated levels of von Willebrand Factor in cirrhosis support platelet adhesion despite reduced functional capacity. Hepatology. 2006;44:53–61. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
