

Radiological Features of Gastrointestinal Lymphoma
- PMID: 26819598
- PMCID: PMC4706984
- DOI: 10.1155/2016/2498143
Radiological Features of Gastrointestinal Lymphoma
Erratum in
-
Corrigendum to "Radiological Features of Gastrointestinal Lymphoma".Gastroenterol Res Pract. 2016;2016:9742102. doi: 10.1155/2016/9742102. Epub 2016 Nov 24. Gastroenterol Res Pract. 2016. PMID: 27999592 Free PMC article.
Abstract
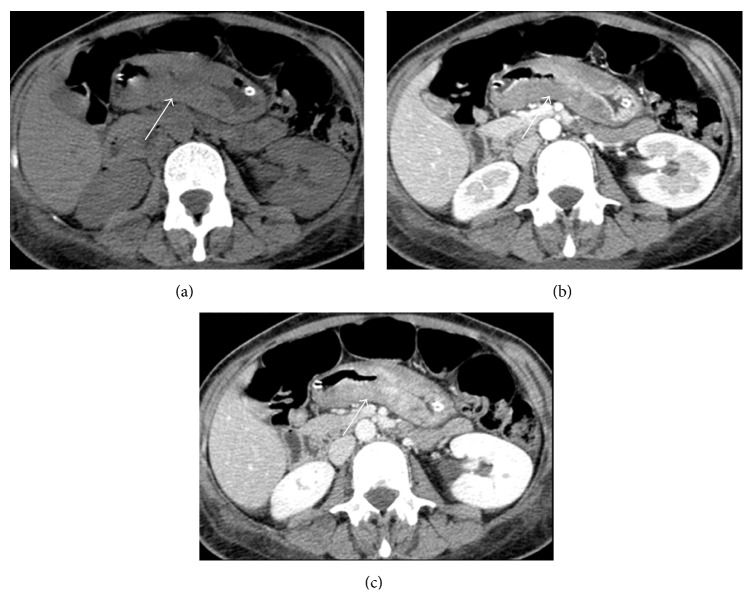
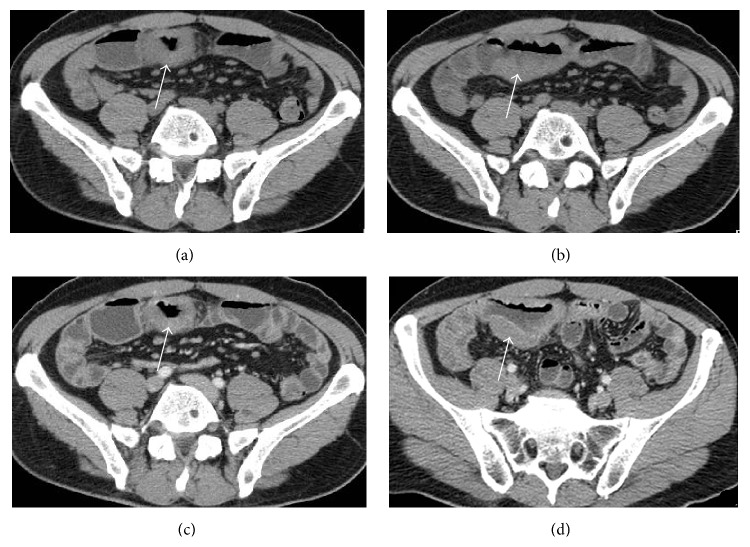
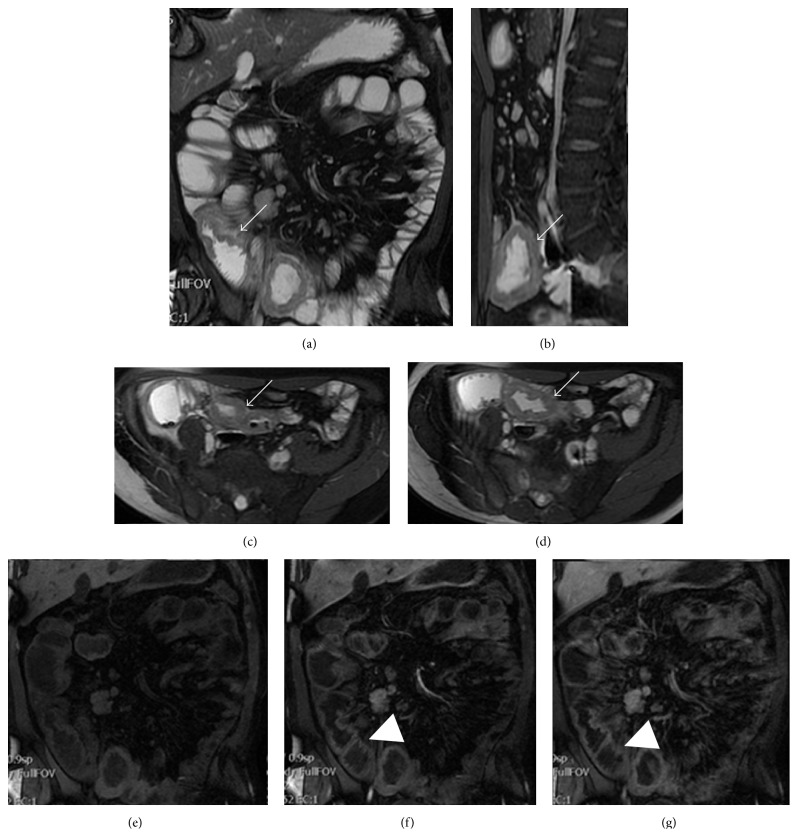
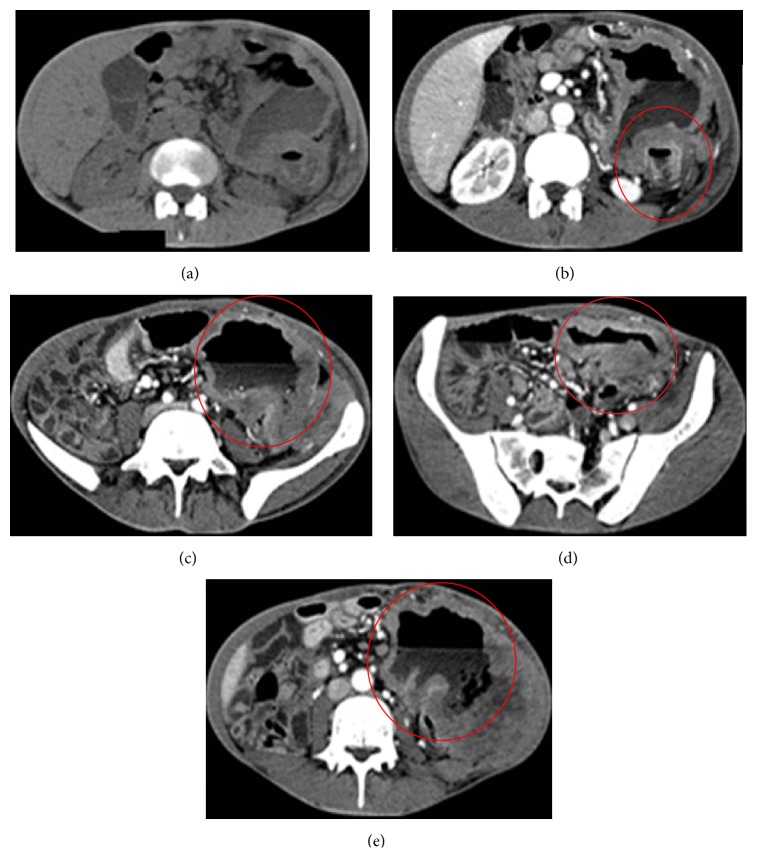
Gastrointestinal lymphomas represent 5-20% of extranodal lymphomas and mainly occur in the stomach and small intestine. Clinical findings are not specific, thus often determining a delay in the diagnosis. Imaging features at conventional and cross-sectional imaging must be known by the radiologist since he/she plays a pivotal role in the diagnosis and disease assessment, thus assisting in the choice of the optimal treatment to patients. This review focuses on the wide variety of imaging presentation of esophageal, gastric, and small and large bowel lymphoma presenting their main imaging appearances at conventional and cross-sectional imaging, mainly focusing on computed tomography and magnetic resonance, helping in the choice of the best imaging technique for the disease characterization and assessment and the recognition of potential complications.
Figures
References
-
- Cupps R. E., Hodgson J. R., Dockerty M. B., Adson M. A. Primary lymphoma in the small intestine: problems of roentgenologic diagnosis. Radiology. 1969;92(6):1354–1362. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
