

Learning Curve of Percutaneous Endoscopic Lumbar Discectomy Based on the Period (Early vs. Late) and Technique (in-and-out vs. in-and-out-and-in): A Retrospective Comparative Study
- PMID: 26819689
- PMCID: PMC4728092
- DOI: 10.3340/jkns.2015.58.6.539
Learning Curve of Percutaneous Endoscopic Lumbar Discectomy Based on the Period (Early vs. Late) and Technique (in-and-out vs. in-and-out-and-in): A Retrospective Comparative Study
Abstract
Objective: To report the learning curve of percutaneous endoscopic lumbar discectomy (PELD) for a surgeon who had not been previously exposed to this procedure based on the period and detailed technique with a retrospective matched comparative design.
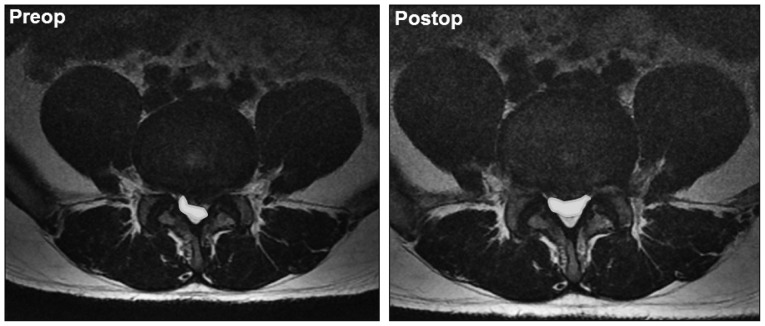
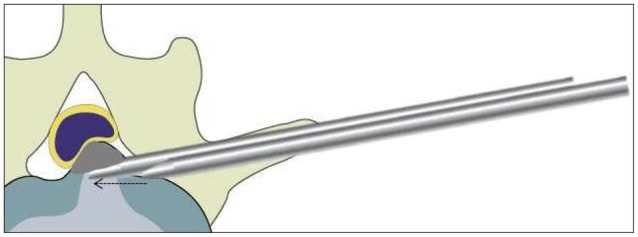
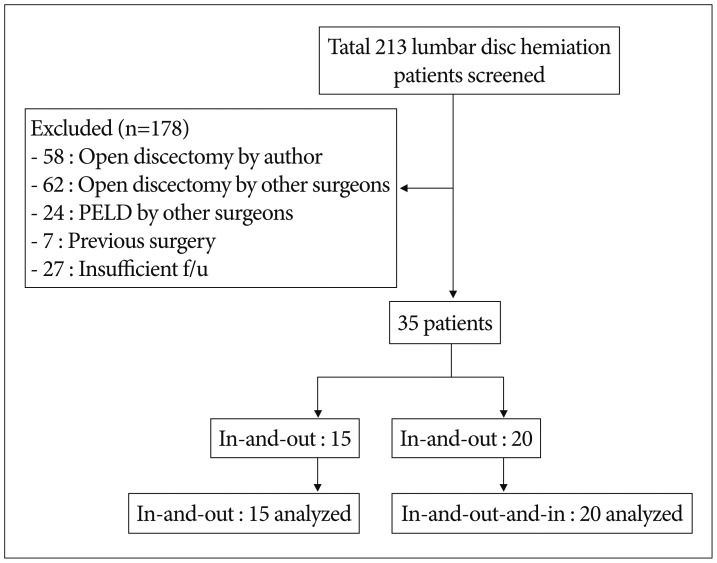
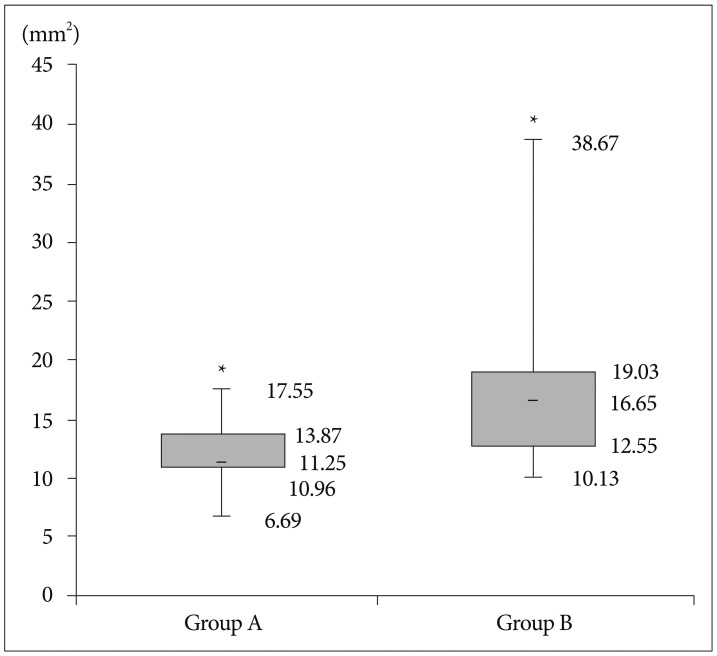
Methods: Of 213 patients with lumbar disc herniation encountered during the reference period, 35 patients who were followed up for 1 year after PELD were enrolled in this study. The patients were categorized by the period and technique of operation : group A, the first 15 cases, who underwent by the 'in-and-out' technique; group B, the next 20 cases, who underwent by the 'in-and-out-and-in' technique. The operation time, failure rate, blood loss, complication rate, re-herniation rate, the Visual Analogue Scale (VAS) for back and leg were checked. The alteration of dural sac cross-sectional area (DSCSA) between the preoperative and the postoperative MRI was checked.
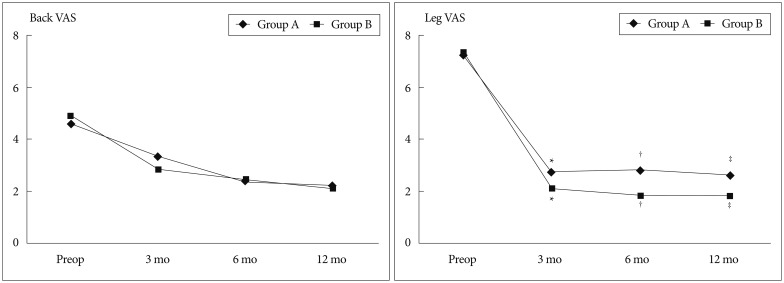
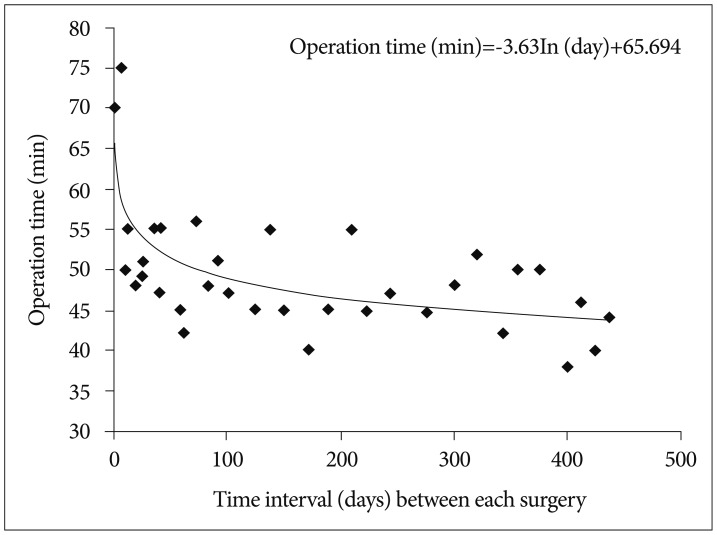
Results: Operative time was rapidly reduced in the early phase, and then tapered to a steady state for the 35 cases receiving the PELD. After surgery, VAS scores for the back and leg were decreased significantly in both groups. Complications occurred in 2 patients in group A and 2 patients in group B. Between the two groups, there were significant differences in operative time, improvement of leg VAS, and expansion of DSCSA.
Conclusion: PELD learning curve seems to be acceptable with sufficient preparation. However, because of their high tendency to delayed operation time, operation failure, and re-herniation, caution should be exercised at the early phase of the procedure.
Keywords: Intervertebral disc herniation; Learning curve; Percutaneous endoscopic lumbar discectomy.
Figures
References
-
- Chae KH, Ju CI, Lee SM, Kim BW, Kim SY, Kim HS. Strategies for noncontained lumbar disc herniation by an endoscopic approach : transforaminal suprapedicular approach, semi-rigid flexible curved probe, and 3-dimensional reconstruction CT with discogram. J Korean Neurosurg Soc. 2009;46:312–316. - PMC - PubMed
-
- Cho JY, Lee SH, Lee HY. Prevention of development of postoperative dysesthesia in transforaminal percutaneous endoscopic lumbar discectomy for intracanalicular lumbar disc herniation : floating retraction technique. Minim Invasive Neurosurg. 2011;54:214–218. - PubMed
-
- Choi G, Kang HY, Modi HN, Prada N, Nicolau RJ, Joh JY, et al. Risk of developing seizure after percutaneous endoscopic lumbar discectomy. J Spinal Disord Tech. 2011;24:83–92. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
