

Clinical Management of Malignant Glaucoma
- PMID: 26819754
- PMCID: PMC4706935
- DOI: 10.1155/2015/283707
Clinical Management of Malignant Glaucoma
Abstract
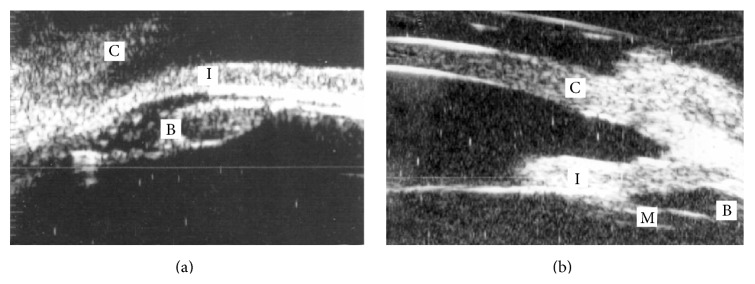
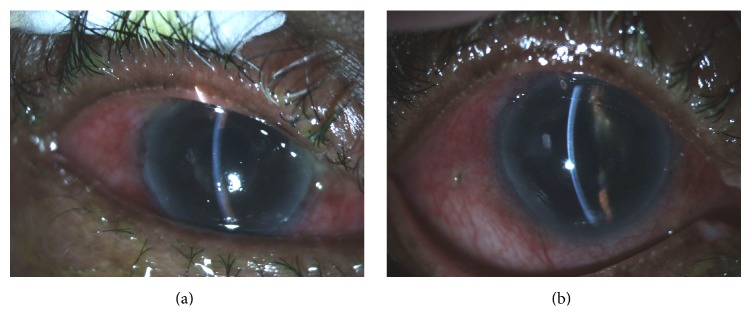
Malignant glaucoma remains one of the most challenging complications of ocular surgery. Although it has been reported to occur spontaneously or after any ophthalmic procedure, it is most commonly encountered after glaucoma surgery in eyes with prior chronic angle closure. The clinical diagnosis is made in the setting of a patent peripheral iridotomy and axial flattening of the anterior chamber. Intraocular pressure is usually elevated, but it may be normal in some cases. Although the exact etiology of this condition is not fully understood, several mechanisms have been proposed and it is thought to result from posterior misdirection of aqueous humor into or behind the vitreous. This review discusses pathophysiology, differential diagnosis, imaging modalities, and current treatment strategies for this rare form of secondary glaucoma.
Figures
References
-
- von Graefe A. Beltrage zur patholoogie and therapie des glaucomas. Albrecht von Graefe. Archives of Ophthalmology. 1869;15, article 108
-
- Reed J. E., Thomas J. V., Lytle R. A., Simmons R. J. Malignant glaucoma induced by an intraocular lens. Ophthalmic Surgery. 1990;21(3):177–180. - PubMed
-
- Duy T. P., Wollensak J. Ciliary block (malignant) glaucoma following posterior chamber lens implantation. Ophthalmic Surgery. 1987;18(10):741–744. - PubMed
-
- Hanish S. J., Lamberg R. L., Gordon J. M. Malignant glaucoma following cataract extraction and intraocular lens implant. Ophthalmic Surgery. 1982;13(9):713–714. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
