

Mycoplasma pneumoniae, a trigger for Weston Hurst syndrome
- PMID: 26819961
- PMCID: PMC4723134
- DOI: 10.1212/NXI.0000000000000187
Mycoplasma pneumoniae, a trigger for Weston Hurst syndrome
Abstract
Objective: We report a case of Mycoplasma pneumoniae infection as one possible trigger for Weston Hurst syndrome (acute hemorrhagic leukoencephalitis), a rare disorder of microvascular injury often described as a postinfectious complication of an upper respiratory illness.
Methods: This is a case of a 27-year-old man presenting with a Glasgow Coma Scale score of 3 and an acute head CT revealing extensive vasogenic edema in the right hemisphere associated with mass effect in the context of a recent upper respiratory illness. Right frontal biopsy was performed on day 2, which showed acute cerebritis, and the patient was aggressively treated with antibiotics. However, over the next 5 days from presentation, the vasogenic edema increased, leading ultimately to brain herniation and death.
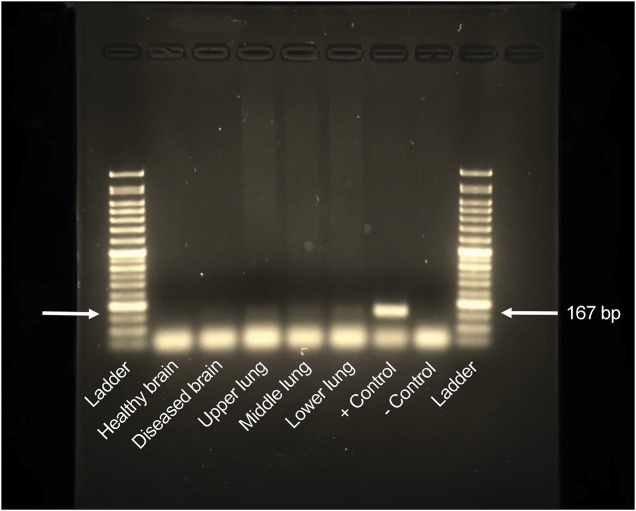
Results: A full autopsy was performed at 5 days from presentation, which showed areas of vessel wall fibrinoid necrosis throughout the right hemisphere as well as, but less so, in the left frontal lobe and pons. Chest x-ray on presentation revealed atypical pneumonia, blood tests were positive for cold agglutinins, and at full autopsy, there was myocarditis, all in keeping with recent M pneumoniae infection. DNA obtained from lung and diseased brain (postmortem) was positive for Mycoplasma providing more direct evidence for brain invasion by this organism as the ultimate trigger for Weston Hurst syndrome.
Conclusions: This is a rare case report of Weston Hurst syndrome having both initial brain biopsy on day 2 and full autopsy results on day 5 of presentation revealing important clinical clues about the pathogenesis of this often fatal disorder.
Figures




References
-
- Dos Santos MP, Martin J, Woulfe J, et al. Autopsy-proven acute hemorrhagic leukoencephalitis in an elderly patient. Can J Neurol Sci 2014;41:99–102. - PubMed
-
- Gillies CG, Grunnet M, Hamilton CW. Tubular inclusions in macrophages in the brain of a patient with acute hemorrhagic leukoencephalitis (Weston Hurst syndrome). Ultrastruct Pathol 1994;18:19–22. - PubMed
-
- Donnet A, Dufour H, Gambarelli D, et al. Acute Weston Hurst necrotizing hemorrhagic leukoencephalitis. Rev Neurol 1996;152:748–751. - PubMed
-
- Tshibanda L, Nchimi A, Otte M, et al. Hurst acute haemorrhagic leukoencephalitis: MRI findings [in French]. JBR-BTR 2007;90:290–293. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases