

Pressure topography metrics for high-resolution pharyngeal-esophageal manofluorography-a normative study of younger and older adults
- PMID: 26822009
- PMCID: PMC4892368
- DOI: 10.1111/nmo.12769
Pressure topography metrics for high-resolution pharyngeal-esophageal manofluorography-a normative study of younger and older adults
Abstract
Background: We aimed to define normative values for novel pressure topography metrics for high-resolution pharyngeal-esophageal manofluorography. The effects of age, gender, and bolus properties were examined.
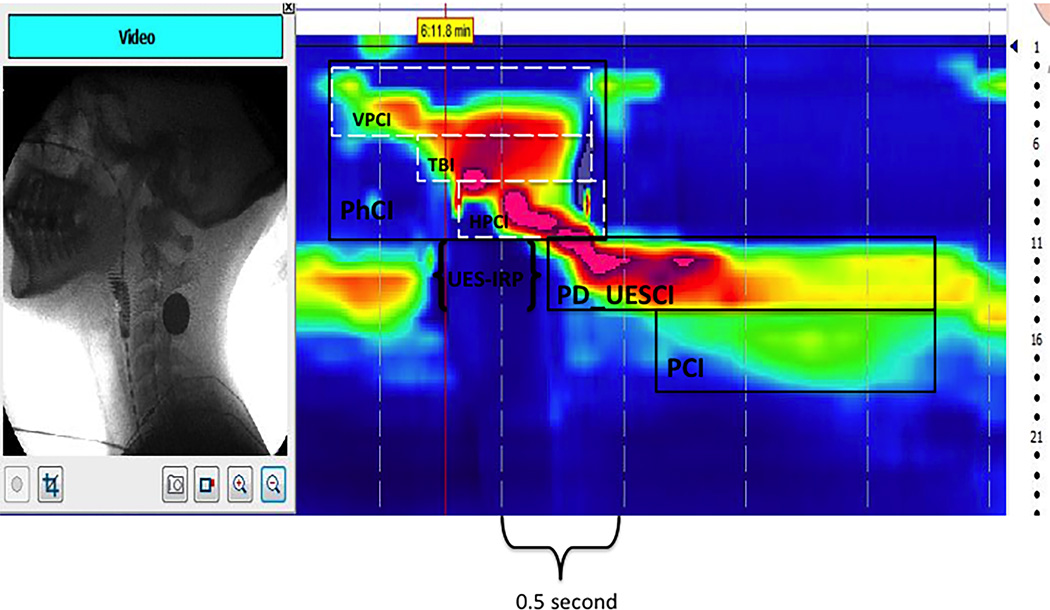
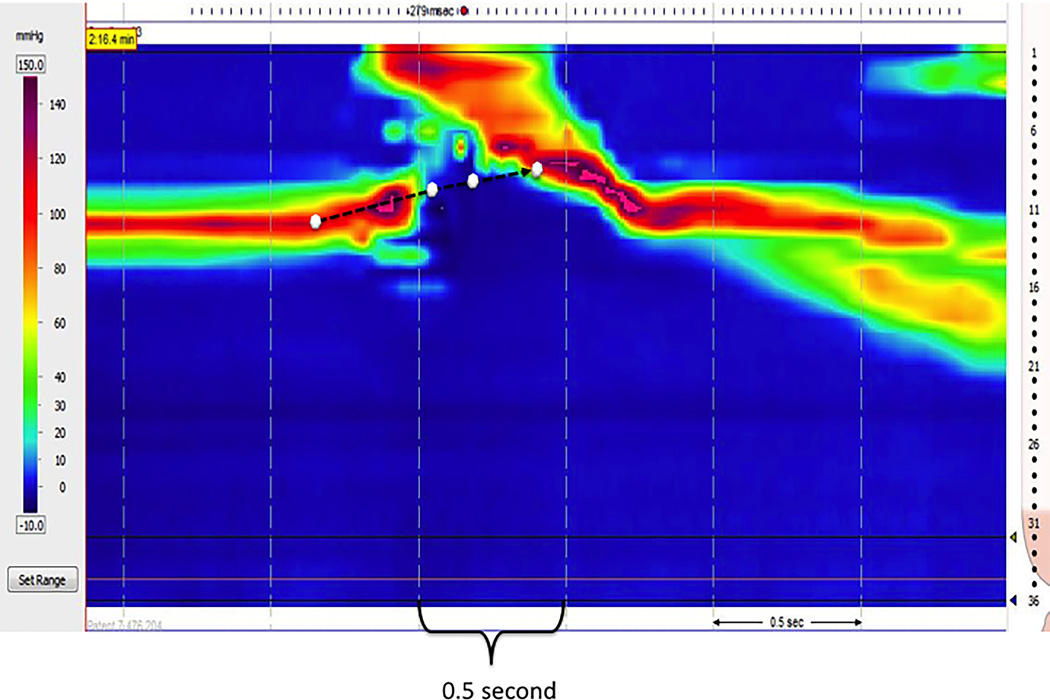
Methods: Concurrent high-resolution manometry (HRM) and videofluoroscopy data were collected from 22 younger (aged 21-40) and 22 older (aged 60-80) healthy subjects. Pressure topography was analyzed by correlating pressure domains with videofluoroscopic events. Nine pressure topography metrics of the pharyngeal and proximal esophageal swallow were extracted; four of these were also compared with previously obtained esophageal HRM studies to assess the effects of catheter diameter.
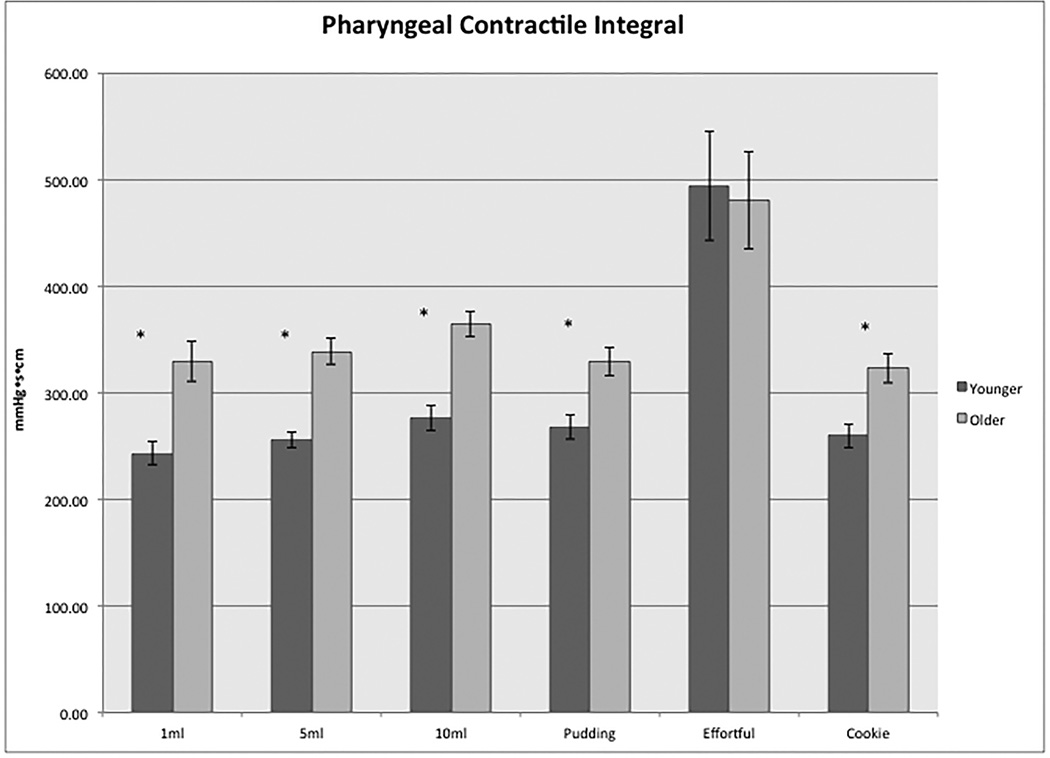
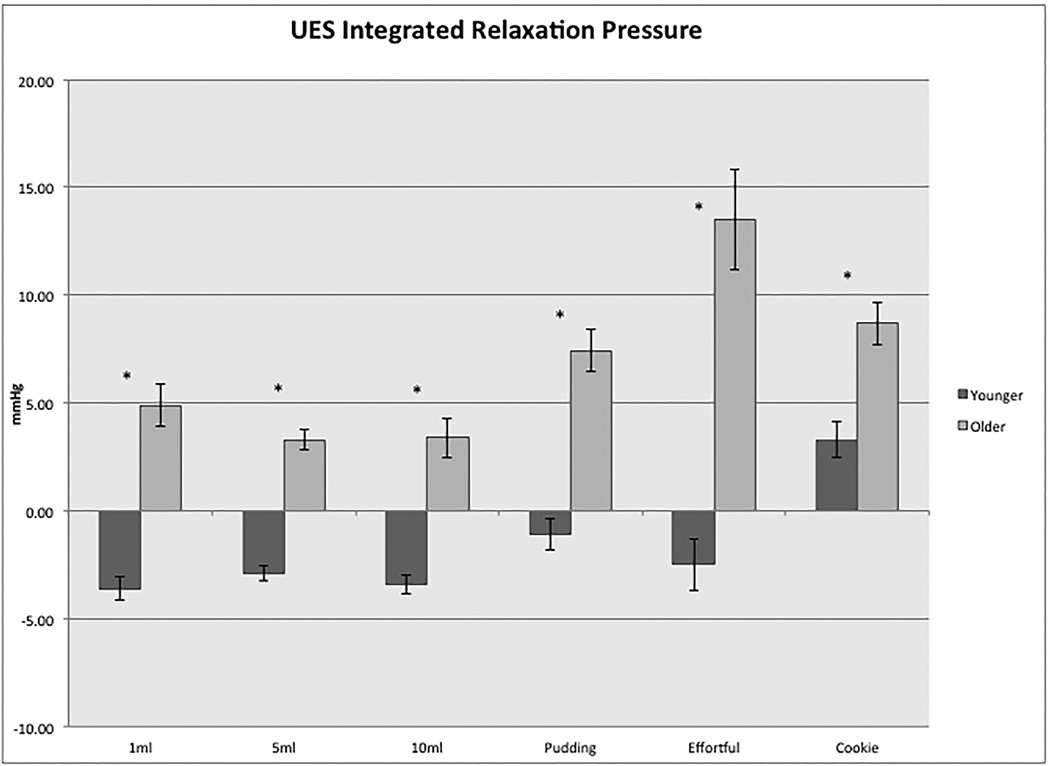
Key results: Older individuals exhibited more vigorous contractility in the pharynx than did younger subjects with all bolus types, but the greatest values for both groups were with effortful swallow and on that measure the age groups were similar. Upper esophageal sphincter (UES) intrabolus pressure during sphincter opening was also greater in the older subjects. Some gender differences were observed, particularly related to proximal esophageal contractile vigor. Bolus consistency had no consistent effect. Studies using the larger catheter diameter resulted in significantly greater contractile vigor in the UES and proximal esophagus.
Conclusions & inferences: Older adults exhibited more vigorous pharyngeal contractions than young adults, albeit within a similar range of capacity, perhaps reflecting a compensatory response to other age-related physiological changes. Greater UES intrabolus pressures observed during bolus transit in the older group likely reflect reduced UES compliance with age. Normative data on novel HRM metrics collected in this study can serve as a reference for future clinical studies.
Keywords: dysphagia; high-resolution manometry; mano-fluorography; pharyngeal swallow; upper esophageal sphincter.
© 2016 John Wiley & Sons Ltd.
Conflict of interest statement
No competing interests declared
Figures
References
-
- Ghosh SK, Pandolfino JE, Zhang Q, Jarosz A, Kahrilas PJ. Deglutitive upper esophageal sphincter relaxation: a study of 75 volunteer subjects using solid-state high-resolution manometry. Am J Physiol Gastrointest Liver Physiol. 2006 Sep;291(3):G525–G531. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
