

Impact of the introduction of EBUS on time to management decision, complications, and invasive modalities used to diagnose and stage lung cancer: a pragmatic pre-post study
- PMID: 26822160
- PMCID: PMC4730595
- DOI: 10.1186/s12885-016-2081-z
Impact of the introduction of EBUS on time to management decision, complications, and invasive modalities used to diagnose and stage lung cancer: a pragmatic pre-post study
Abstract
Background: Utilisation of endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) and guide sheath (EBUS-GS) for diagnosis and staging of lung cancer is gaining popularity, however, its impact on clinical practice is unclear. This study aimed to determine the impact of the introduction of endobronchial ultrasound-guided procedures (EBUS) on time to management decision for lung cancer patients, and on the utilisation of other invasive diagnostic modalities, including CT-guided trans-thoracic needle aspiration (CT-TTNA), bronchoscopy, and mediastinoscopy.
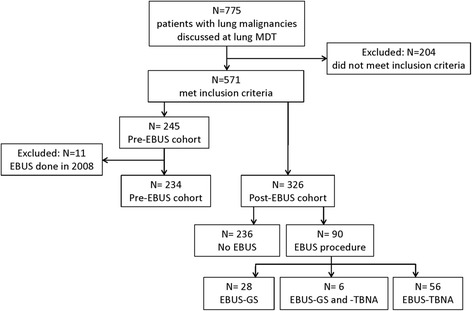
Methods: Hospital records of new primary lung cancer patients presenting in 2007 and 2008 (Pre-EBUS cohort) and in 2010 and 2011 (Post-EBUS cohort) were reviewed retrospectively.
Results: The Pre-EBUS cohort included 234 patients. Of the 326 patients in the Post-EBUS cohort, 90 had an EBUS procedure (EBUS-TBNA for 19.0% and EBUS-GS for 10.4% of cases). The number of CT-TTNAs and bronchoscopies decreased following the introduction of EBUS (p = 0.015 and p < 0.001 respectively). Of 162 CT-TTNAs, 59 (36%) resulted in complications compared to 1 complication each for bronchoscopy and EBUS-GS, and no complications from EBUS-TBNA. Fewer complications occurred overall in the Post-EBUS cohort compared to the Pre-EBUS cohort (p = 0.0264). The median time to management decision was 17 days (IQR 24) for the Pre-EBUS and 13 days (IQR 21) for the Post-EBUS cohort (p = 0.07). Within the Post-EBUS cohort, median time to management decision was longer for the EBUS group (n = 90) than the Non-EBUS group (17 days (IQR 29) vs. 10 days (IQR 10), p < 0.001). For half of EBUS-TBNA patients (n = 28, 50.0%) and EBUS-GS patients (n = 14, 50.0 %), EBUS alone provided sufficient diagnostic and/or staging information; these patients had median time to management decision of 10 days. Regression analysis revealed that the number of imaging events, inpatient, and outpatient visits were significant predictors of time to management decision of >28 days; EBUS was not a predictor of time to management decision.
Conclusions: The introduction of EBUS led to fewer CT-TTNAs and bronchoscopies and did not impact on the time to management decision. EBUS-TBNA or EBUS-GS alone provided sufficient information for diagnosis and/or regional staging in half of the lung cancer patients referred for this investigation.
References
-
- Travis WD, Brambilla E, Noguchi M, Nicholson AG, Geisinger KR, Yatabe Y, et al. International association for the study of lung cancer/american thoracic society/european respiratory society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011;6(2):244–85. doi: 10.1097/JTO.0b013e318206a221. - DOI - PMC - PubMed
-
- Adamson RT. Biomarkers and molecular profiling in non-small cell lung cancer: an expanding role and its managed care implications. Am J Manag Care. 2013;19(19 Suppl):s398–404. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
