

Use and Outcomes of Minimally Invasive Lobectomy for Stage I Non-Small Cell Lung Cancer in the National Cancer Data Base
- PMID: 26822346
- PMCID: PMC4763985
- DOI: 10.1016/j.athoracsur.2015.11.018
Use and Outcomes of Minimally Invasive Lobectomy for Stage I Non-Small Cell Lung Cancer in the National Cancer Data Base
Abstract
Background: Previous studies have raised concerns that video-assisted thoracoscopic (VATS) lobectomy may compromise nodal evaluation. The advantages or limitations of robotic lobectomy have not been thoroughly evaluated.
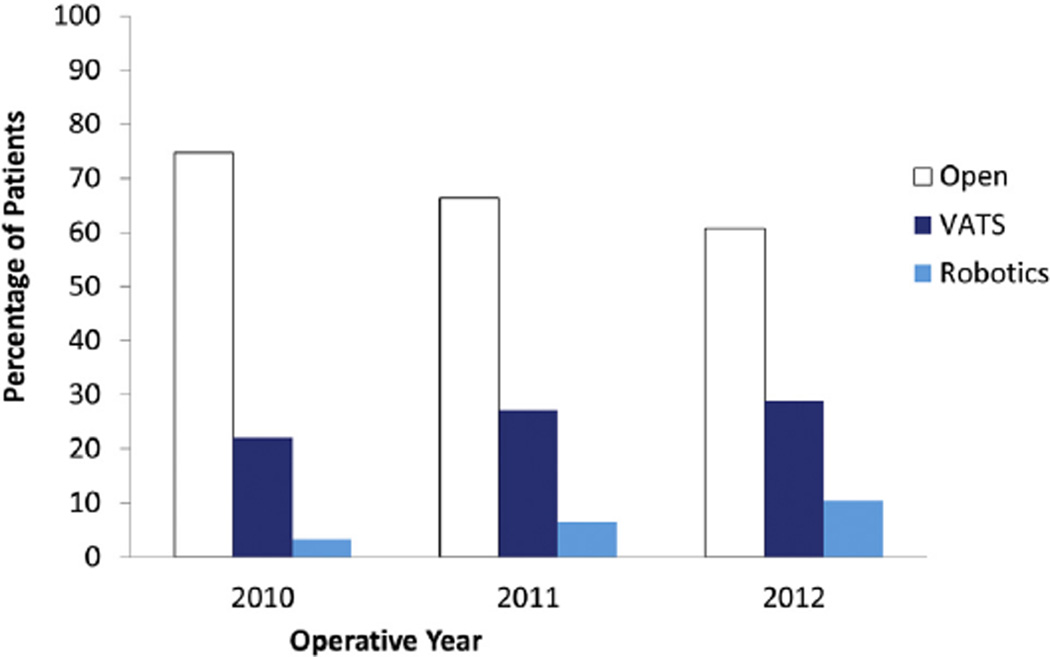
Methods: Perioperative outcomes and survival of patients who underwent open versus minimally-invasive surgery (MIS [VATS and robotic]) lobectomy and VATS versus robotic lobectomy for clinical T1-2, N0 non-small cell lung cancer from 2010 to 2012 in the National Cancer Data Base were evaluated using propensity score matching.
Results: Of 30,040 lobectomies, 7,824 were VATS and 2,025 were robotic. After propensity score matching, when compared with the open approach (n = 9,390), MIS (n = 9,390) was found to have increased 30-day readmission rates (5% versus 4%, p < 0.01), shorter median hospital length of stay (5 versus 6 days, p < 0.01), and improved 2-year survival (87% versus 86%, p = 0.04). There were no significant differences in nodal upstaging and 30-day mortality between the two groups. After propensity score matching, when compared with the robotic group (n = 1,938), VATS (n = 1,938) was not significantly different from robotics with regard to nodal upstaging, 30-day mortality, and 2-year survival.
Conclusions: In this population-based analysis, MIS (VATS and robotic) lobectomy was used in the minority of patients for stage I non-small cell lung cancer. MIS lobectomy was associated with shorter length of hospital stay and was not associated with increased perioperative mortality, compromised nodal evaluation, or reduced short-term survival when compared with the open approach. These results suggest the need for broader implementation of MIS techniques.
Copyright © 2016 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
A National Analysis of Long-term Survival Following Thoracoscopic Versus Open Lobectomy for Stage I Non-small-cell Lung Cancer.Ann Surg. 2019 Jan;269(1):163-171. doi: 10.1097/SLA.0000000000002342. Ann Surg. 2019. PMID: 28799982
-
Long-term Survival Based on the Surgical Approach to Lobectomy For Clinical Stage I Nonsmall Cell Lung Cancer: Comparison of Robotic, Video-assisted Thoracic Surgery, and Thoracotomy Lobectomy.Ann Surg. 2017 Feb;265(2):431-437. doi: 10.1097/SLA.0000000000001708. Ann Surg. 2017. PMID: 28059973 Free PMC article.
-
A National Analysis of Short-term Outcomes and Long-term Survival Following Thoracoscopic Versus Open Lobectomy for Clinical Stage II Non-Small-Cell Lung Cancer.Ann Surg. 2021 Mar 1;273(3):595-605. doi: 10.1097/SLA.0000000000003231. Ann Surg. 2021. PMID: 30946089
-
In patients with resectable non-small-cell lung cancer, is video-assisted thoracoscopic segmentectomy an appropriate alternative to video-assisted thoracoscopic lobectomy?Interact Cardiovasc Thorac Surg. 2016 Nov;23(5):826-831. doi: 10.1093/icvts/ivw202. Epub 2016 Jul 11. Interact Cardiovasc Thorac Surg. 2016. PMID: 27401084 Review.
-
Video-assisted thoracic surgery lobectomy (VATS), open thoracotomy, and the robot for lung cancer.Ann Thorac Surg. 2008 Feb;85(2):S710-5. doi: 10.1016/j.athoracsur.2007.09.055. Ann Thorac Surg. 2008. PMID: 18222202 Review.
Cited by
-
Perioperative mortality and morbidity after sublobar versus lobar resection for early-stage non-small-cell lung cancer: post-hoc analysis of an international, randomised, phase 3 trial (CALGB/Alliance 140503).Lancet Respir Med. 2018 Dec;6(12):915-924. doi: 10.1016/S2213-2600(18)30411-9. Epub 2018 Nov 12. Lancet Respir Med. 2018. PMID: 30442588 Free PMC article. Clinical Trial.
-
VATS lobectomy for early lung cancer: long-term outcomes.Ann Transl Med. 2019 Sep;7(Suppl 6):S235. doi: 10.21037/atm.2019.08.32. Ann Transl Med. 2019. PMID: 31656814 Free PMC article. No abstract available.
-
Predictive factors of postoperative complications in single-port video-assisted thoracoscopic anatomical resection: Two center experience.Medicine (Baltimore). 2018 Oct;97(40):e12664. doi: 10.1097/MD.0000000000012664. Medicine (Baltimore). 2018. PMID: 30290649 Free PMC article.
-
Minimally invasive thoracic surgery: robot-assisted versus video-assisted thoracoscopic surgery.Wideochir Inne Tech Maloinwazyjne. 2023 Sep;18(3):436-444. doi: 10.5114/wiitm.2023.128714. Epub 2023 Jun 20. Wideochir Inne Tech Maloinwazyjne. 2023. PMID: 37868280 Free PMC article. Review.
-
International expert consensus on the management of bleeding during VATS lung surgery.Ann Transl Med. 2019 Dec;7(23):712. doi: 10.21037/atm.2019.11.142. Ann Transl Med. 2019. PMID: 32042728 Free PMC article. Review.
References
-
- Yan TD, Black D, Bannon PG, McCaughan BC. Systematic review and meta-analysis of randomized and non-randomized trials on safety and efficacy of video-assisted thoracic surgery lobectomy for early-stage non-small-cell lung cancer. J Clin Oncol. 2009;27:2553–2562. - PubMed
-
- Mathisen DJ. Is video-assisted thoracoscopic lobectomy inferior to open lobectomy oncologically? Ann Thorac Surg. 2013;96:755–756. - PubMed
-
- Wilson JL, Louie BE, Cerfolio RJ, et al. The prevalence of nodal upstaging during robotic lung resection in early stage non-small cell lung cancer. Ann Thorac Surg. 2014;97:1901–1907. - PubMed
-
- Nasir BS, Bryant AS, Minnich DJ, Wei B, Cerfolio RJ. Performing robotic lobectomy and segmentectomy: cost, profitability, and outcomes. Ann Thorac Surg. 2014;98:203–209. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
