

Spinal arteriovenous fistulae in patients with hereditary hemorrhagic telangiectasia: A case report and systematic review of the literature
- PMID: 26823330
- PMCID: PMC4984358
- DOI: 10.1177/1591019915623560
Spinal arteriovenous fistulae in patients with hereditary hemorrhagic telangiectasia: A case report and systematic review of the literature
Abstract
Background: Although rare, spinal arteriovenous malformations (AVMs) are thought to be more prevalent in the hereditary Hereditary Hemorrhagic Telangiectasia (HHT) population.
Methods: We report a case of a spinal AVM in a 37-year-old female with HHT treated with endovascular embolization. In addition, we report findings from a systematic review of the literature on the clinical characteristics, angioarchitecture, and clinical outcomes of HHT patients with spinal AVMs.
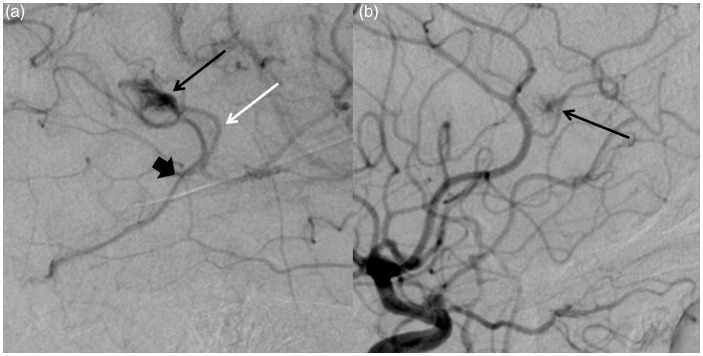
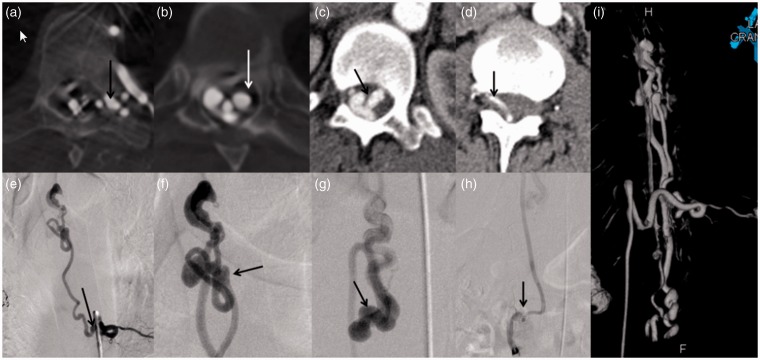
Results: The patient is a 37 year-old female with definite HHT who presented with a one-year history of progressive gait difficulty. The spinal fistula was incidentally detected on chest computed tomography (CT). Spinal angiography demonstrated a large perimedullary arteriovenous fistula was supplied by a posterolateral spinal artery. The fistula was treated with detachable coils. The patient made a complete neurological recovery. Our systematic review yielded 25 additional cases of spinal AVMs in HHT patients. All fistulae were perimedullary (100.0%). Treatments were described in 24 of the 26 lesions. Endovascular-only treatment was performed in 16 cases (66.6%) and surgical-only treatment was performed in five cases (20.8%). Complete or near-complete occlusion rates were 86.7% (13/15) for endovascular treated cases, 100.0% (4/4) for surgery and 66.6% (2/3) for combined treatments. Overall, 80.0% of patients (16/20) reported improvement in function following treatment, 100.0% (5/5) in the surgery group and 84.6% (11/13) reported improvement in the endovascular group.
Conclusions: Spinal fistulae in HHT patients are usually type IV perimedullary fistulae. Both endovascular and surgical treatments appeared to be effective in treating these lesions. However, it is clear that endovascular therapy has become the preferred treatment modality.
Keywords: Hereditary hemorrhagic telangiectasia; spinal fistula.
© The Author(s) 2016.
Figures

Similar articles
-
Probiotics and infective endocarditis in patients with hereditary hemorrhagic telangiectasia: a clinical case and a review of the literature.BMC Infect Dis. 2018 Feb 1;18(1):65. doi: 10.1186/s12879-018-2956-5. BMC Infect Dis. 2018. PMID: 29390976 Free PMC article.
-
Interdisciplinary treatment algorithm for facial high-flow arteriovenous malformations, and review of the literature.J Craniomaxillofac Surg. 2018 May;46(5):765-772. doi: 10.1016/j.jcms.2018.03.002. Epub 2018 Mar 9. J Craniomaxillofac Surg. 2018. PMID: 29609843
-
Comparative analysis of spinal extradural arteriovenous fistulas with or without intradural venous drainage: a systematic literature review.Neurosurg Focus. 2012 May;32(5):E8. doi: 10.3171/2012.2.FOCUS1216. Neurosurg Focus. 2012. PMID: 22537134
-
Sclerotherapy for Hereditary Hemorrhagic Telangiectasia-Related Epistaxis: A Systematic Review.Ann Otol Rhinol Laryngol. 2023 Jan;132(1):82-90. doi: 10.1177/00034894221078075. Epub 2022 Feb 12. Ann Otol Rhinol Laryngol. 2023. PMID: 35152768
-
A rapid and systematic review of the clinical effectiveness and cost-effectiveness of topotecan for ovarian cancer.Health Technol Assess. 2001;5(28):1-110. doi: 10.3310/hta5280. Health Technol Assess. 2001. PMID: 11701100
Cited by
-
Anaesthetic management for caesarean section in a patient with hereditary haemorrhagic telangiectasia and severe epistaxis during pregnancy.BMJ Case Rep. 2023 Oct 3;16(10):e255530. doi: 10.1136/bcr-2023-255530. BMJ Case Rep. 2023. PMID: 37788916 Free PMC article.
-
Spinal Arteriovenous Fistula, A Manifestation of Hereditary Hemorrhagic Telangiectasia: A Case Report.Clin Pract Cases Emerg Med. 2020 Aug;4(3):417-420. doi: 10.5811/cpcem.2020.5.47086. Clin Pract Cases Emerg Med. 2020. PMID: 32926701 Free PMC article.
-
Spinal Extramedullary Arteriovenous Fistulas: A 15-Year Endovascular Treatment Experience in a Tertiary Care Hospital in Thailand.Int J Spine Surg. 2023 Aug;17(4):570-578. doi: 10.14444/8446. Epub 2023 Apr 13. Int J Spine Surg. 2023. PMID: 37055176 Free PMC article.
-
A rare case of spinal involvement in hereditary hemorrhagic telangiectasia.Spinal Cord Ser Cases. 2024 Jul 17;10(1):49. doi: 10.1038/s41394-024-00662-1. Spinal Cord Ser Cases. 2024. PMID: 39019878 Free PMC article.
-
Systemic and CNS manifestations of inherited cerebrovascular malformations.Clin Imaging. 2021 Jul;75:55-66. doi: 10.1016/j.clinimag.2021.01.020. Epub 2021 Jan 20. Clin Imaging. 2021. PMID: 33493737 Free PMC article. Review.
References
-
- Shovlin CL, Guttmacher AE, Buscarini E, et al. Diagnostic criteria for hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber syndrome). Am J Med Genet 2000; 91: 66–67. - PubMed
-
- Faughnan ME, Palda VA, Garcia-Tsao G, et al. International guidelines for the diagnosis and management of hereditary haemorrhagic telangiectasia. J Med Genet 2011; 48: 73–87. - PubMed
-
- Kalani MY, Ahmed AS, Martirosyan NL, et al. Surgical and endovascular treatment of pediatric spinal arteriovenous malformations. World Neurosurg 2012; 78: 348–354. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
