

Complete resection of contrast-enhancing tumor volume is associated with improved survival in recurrent glioblastoma-results from the DIRECTOR trial
- PMID: 26823503
- PMCID: PMC4799687
- DOI: 10.1093/neuonc/nov326
Complete resection of contrast-enhancing tumor volume is associated with improved survival in recurrent glioblastoma-results from the DIRECTOR trial
Abstract
Background: The role of reoperation for recurrent glioblastoma (GBM) remains unclear. Prospective studies are lacking. Here, we studied the association of clinical outcome with extent of resection upon surgery for recurrent GBM in the patient cohort of DIRECTOR, a prospective randomized multicenter trial comparing 2 dose-intensified temozolomide regimens at recurrence of GBM.
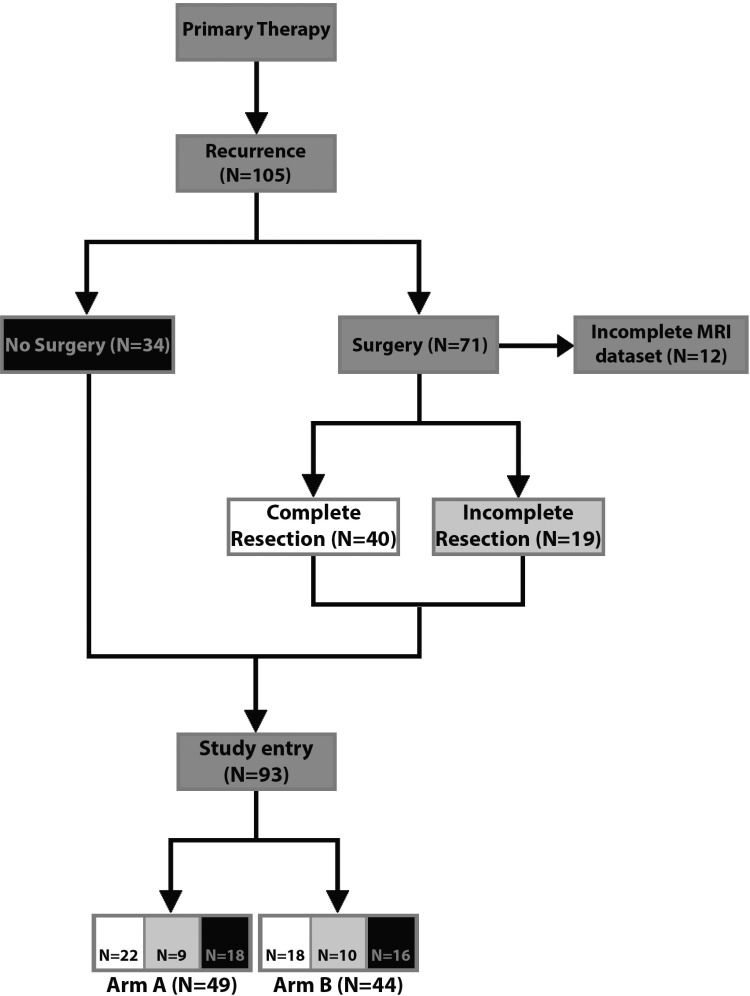
Methods: We analyzed prospectively collected clinical and imaging data from the DIRECTOR cohort (N = 105). Volumetric analysis was performed on gadolinium contrast-enhanced MRI as well as fluid attenuated inversion recovery/T2 MRI and correlated with PFS after initial progression (PFS2) and post-recurrence survival (PRS). Quality of life was monitored by the EORTC QLQ-C30 and QLQ-BN20 questionnaires at 8-week intervals.
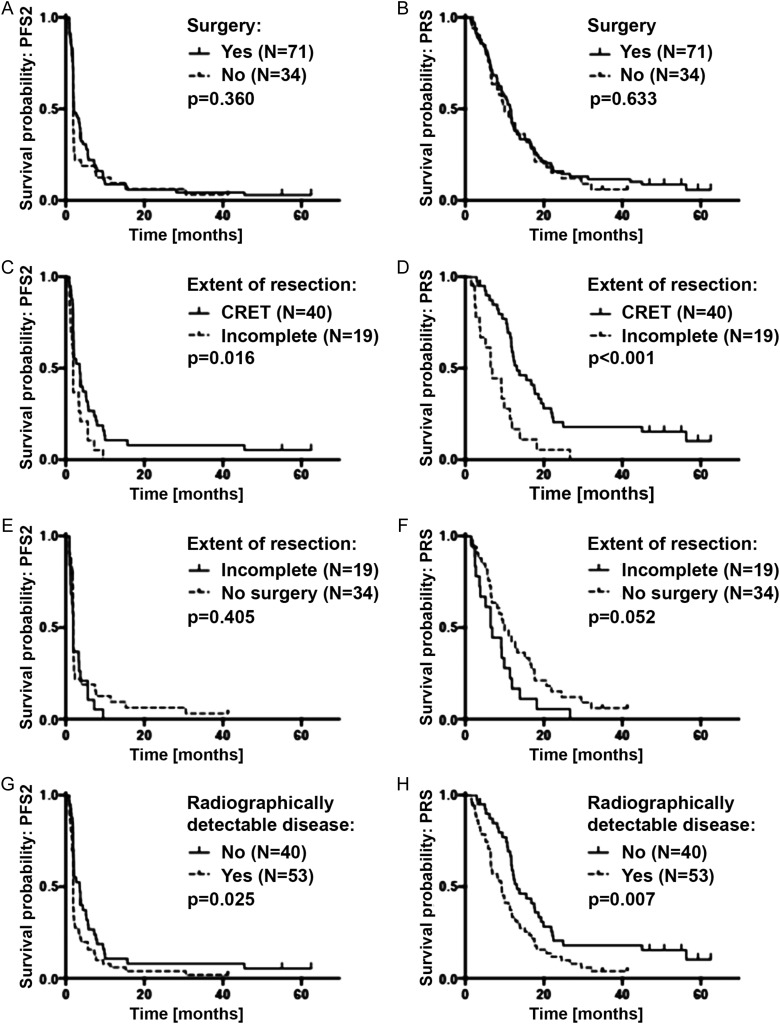
Results: Seventy-one patients received surgery at first recurrence. Prognostic factors, including age, MGMT promoter methylation, and Karnofsky performance score, were balanced between patients with and without reoperation. Outcome in patients with versus without surgery at recurrence was similar for PFS2 (2.0 mo vs 1.9 mo, P = .360) and PRS (11.4 mo vs 9.8 mo, P = .633). Among reoperated patients, post-surgery imaging was available in 59 cases. In these patients, complete resection of contrast-enhancing tumor (N = 40) versus residual detection of contrast enhancement (N = 19) was associated with improved PRS (12.9 mo [95% CI: 11.5-18.2] vs 6.5 mo [95% CI: 3.6-9.9], P < .001) and better quality of life. Incomplete tumor resection was associated with inferior PRS compared with patients who did not undergo surgery (6.5 vs 9.8 mo, P = .052). Quality of life was similar in these 2 groups.
Conclusion: Surgery at first recurrence of GBM improves outcome if complete resection of contrast-enhancing tumor is achieved.
Keywords: DIRECTOR; outcome; re-operation; recurrent GBM; volumetry.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Weller M, van den Bent M, Hopkins K, et al. EANO guideline for the diagnosis and treatment of anaplastic gliomas and glioblastoma. Lancet Oncol. 2014;15(9):e395–e403. - PubMed
-
- Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med. 2005;352(10):987–996. - PubMed
-
- Stupp R, Hegi ME, Gorlia T, et al. Cilengitide combined with standard treatment for patients with newly diagnosed glioblastoma with methylated MGMT promoter (CENTRIC EORTC 26071-22072 study): a multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2014;15(10):1100–1108. - PubMed
-
- Chinot OL, Wick W, Mason W, et al. Bevacizumab plus radiotherapy-temozolomide for newly diagnosed glioblastoma. N Engl J Med. 2014;370(8):709–722. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
