

Ketoanalogue-Supplemented Vegetarian Very Low-Protein Diet and CKD Progression
- PMID: 26823552
- PMCID: PMC4926970
- DOI: 10.1681/ASN.2015040369
Ketoanalogue-Supplemented Vegetarian Very Low-Protein Diet and CKD Progression
Abstract
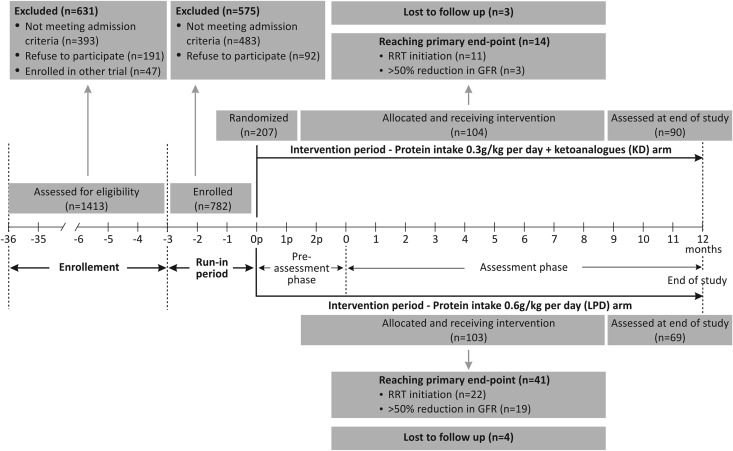
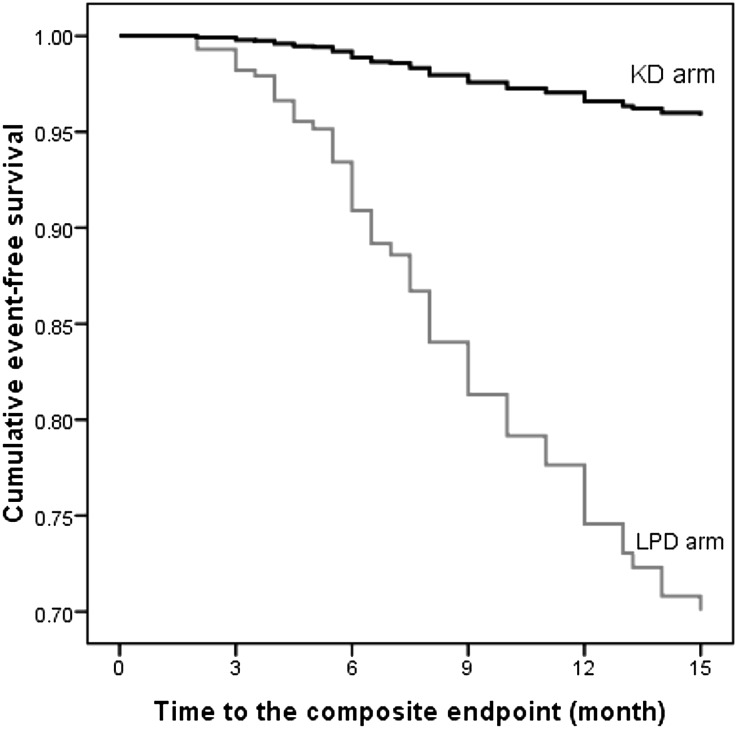
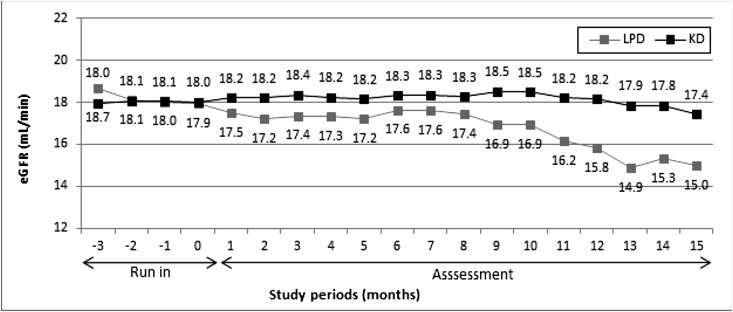
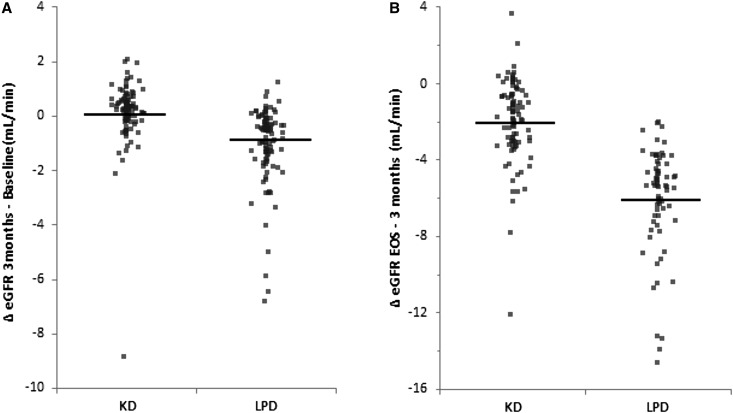
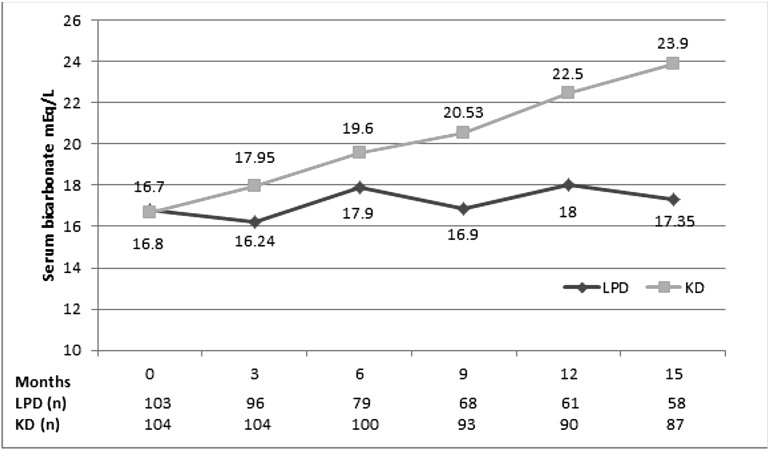
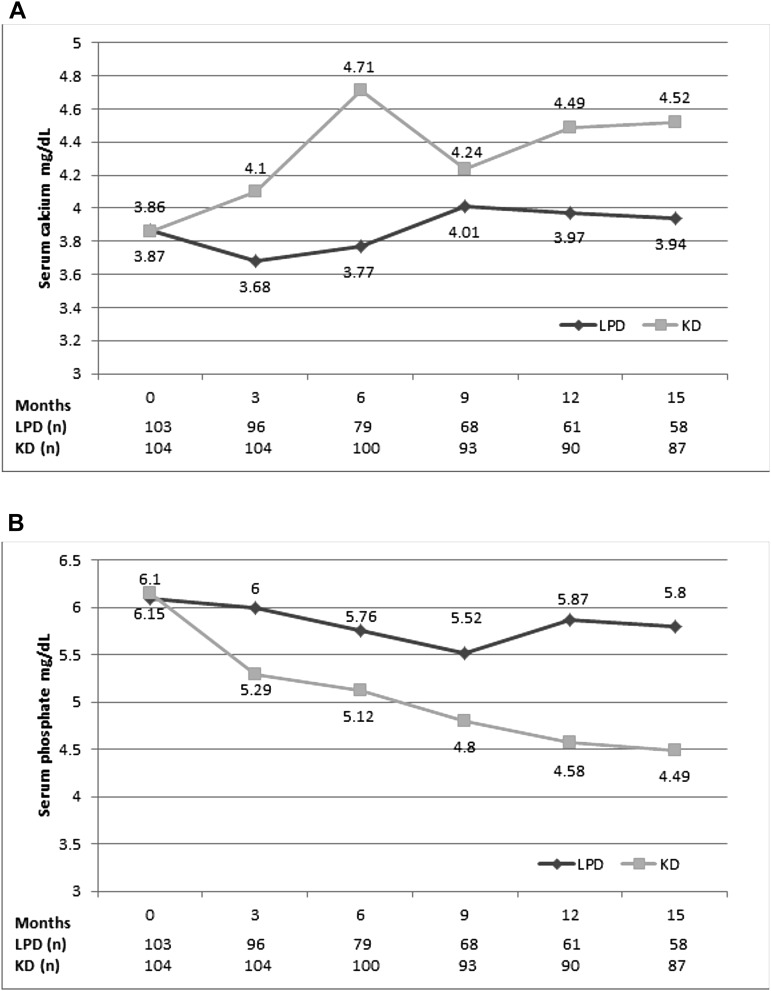
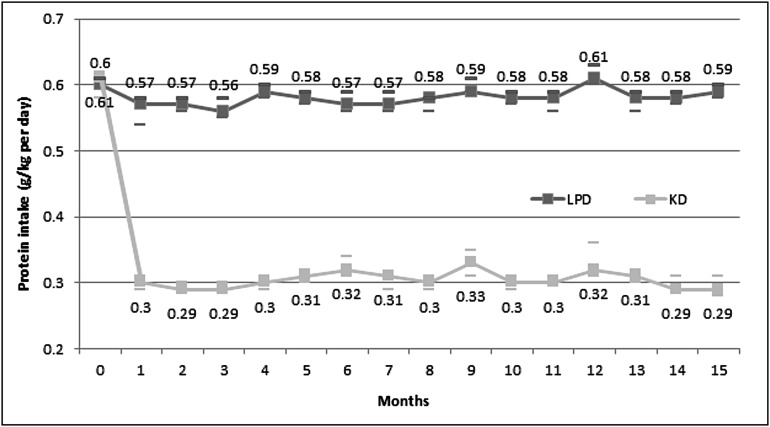
Dietary protein restriction may improve determinants of CKD progression. However, the extent of improvement and effect of ketoanalogue supplementation are unclear. We conducted a prospective, randomized, controlled trial of safety and efficacy of ketoanalogue-supplemented vegetarian very low-protein diet (KD) compared with conventional low-protein diet (LPD). Primary end point was RRT initiation or >50% reduction in initial eGFR. Nondiabetic adults with stable eGFR<30 ml/min per 1.73 m(2), proteinuria <1 g/g urinary creatinine, good nutritional status, and good diet compliance entered a run-in phase on LPD. After 3 months, compliant patients were randomized to KD (0.3 g/kg vegetable proteins and 1 cps/5 kg ketoanalogues per day) or continue LPD (0.6 g/kg per day) for 15 months. Only 14% of screened patients patients were randomized, with no differences between groups. Adjusted numbers needed to treat (NNTs; 95% confidence interval) to avoid composite primary end point in intention to treat and per-protocol analyses in one patient were 4.4 (4.2 to 5.1) and 4.0 (3.9 to 4.4), respectively, for patients with eGFR<30 ml/min per 1.73 m(2) Adjusted NNT (95% confidence interval) to avoid dialysis was 22.4 (21.5 to 25.1) for patients with eGFR<30 ml/min per 1.73 m(2) but decreased to 2.7 (2.6 to 3.1) for patients with eGFR<20 ml/min per 1.73 m(2) in intention to treat analysis. Correction of metabolic abnormalities occurred only with KD. Compliance to diet was good, with no changes in nutritional parameters and no adverse reactions. Thus, this KD seems nutritionally safe and could defer dialysis initiation in some patients with CKD.
Keywords: nutrition; phosphate binders; progression of chronic renal failure; renal function decline.
Copyright © 2016 by the American Society of Nephrology.
Figures
Comment in
-
Dietary Protein as Kidney Protection: Quality or Quantity?J Am Soc Nephrol. 2016 Jul;27(7):1877-9. doi: 10.1681/ASN.2015111286. Epub 2016 Jan 28. J Am Soc Nephrol. 2016. PMID: 26823549 Free PMC article. No abstract available.
References
-
- Bellizzi V, Di Iorio BR, De Nicola L, Minutolo R, Zamboli P, Trucillo P, Catapano F, Cristofano C, Scalfi L, Conte G ERIKA Study-group : Very low protein diet supplemented with ketoanalogs improves blood pressure control in chronic kidney disease. Kidney Int 71: 245–251, 2007 - PubMed
-
- Gansevoort RT, de Zeeuw D, de Jong PE: Additive antiproteinuric effect of ACE inhibition and a low-protein diet in human renal disease. Nephrol Dial Transplant 10: 497–504, 1995 - PubMed
-
- Chauveau P, Combe C, Rigalleau V, Vendrely B, Aparicio M: Restricted protein diet is associated with decrease in proteinuria: Consequences on the progression of renal failure. J Ren Nutr 17: 250–257, 2007 - PubMed
-
- Ikizler TA: Dietary protein restriction in CKD: The debate continues. Am J Kidney Dis 53: 189–191, 2009 - PubMed
-
- Kidney Disease: Improving Global Outcomes : KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int 3: 5–10, 2013 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
