

Epistaxis and pituitary apoplexy due to ruptured internal carotid artery aneurysm embedded within pituitary adenoma
- PMID: 26823732
- PMCID: PMC4713518
Epistaxis and pituitary apoplexy due to ruptured internal carotid artery aneurysm embedded within pituitary adenoma
Abstract
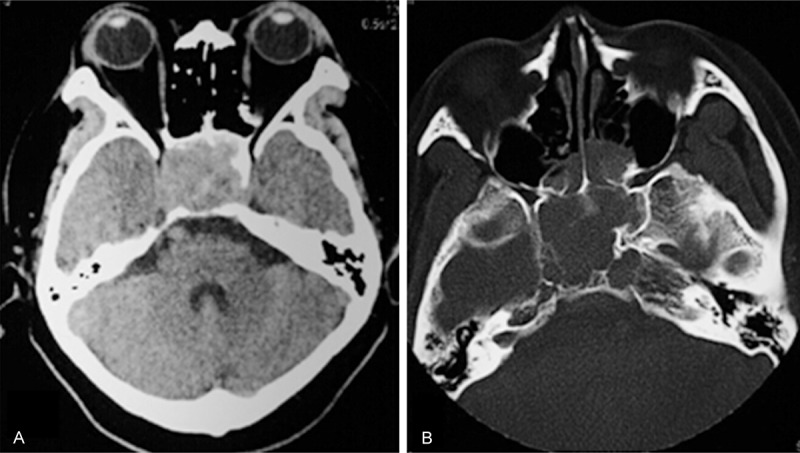
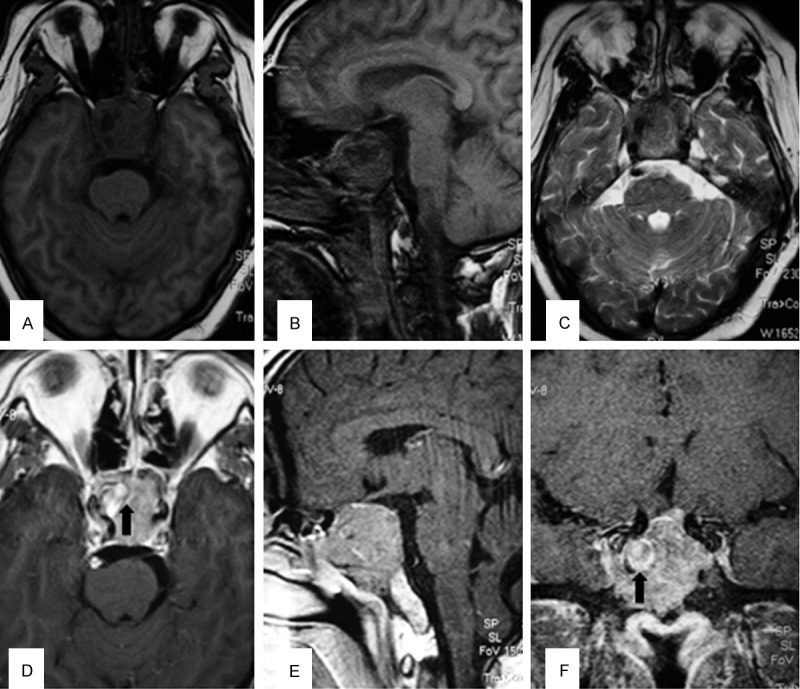
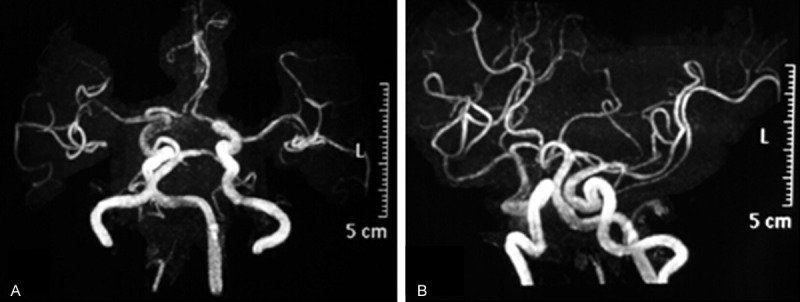
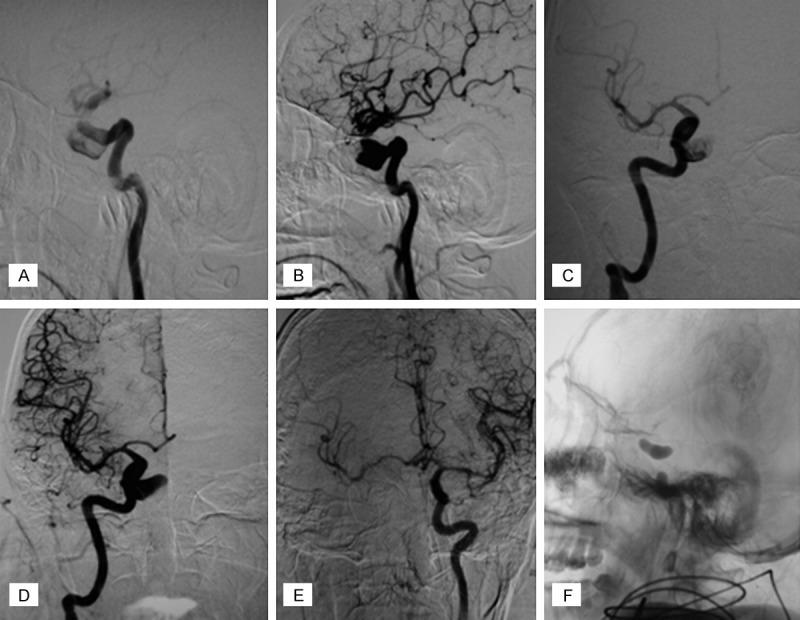
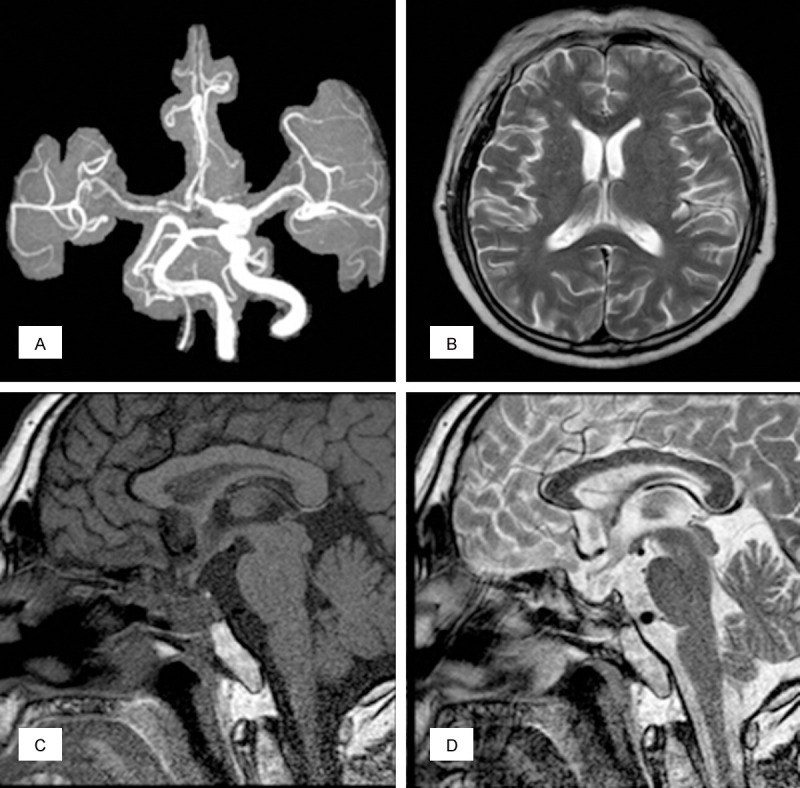
Epistaxis due to ruptured internal carotid artery (ICA) aneurysm embedded within a pituitary adenoma (PA) has seldom been reported in the literature. Here we want to elaborate the incidence, mechanisms, clinical manifestations, and treatment strategy for this condition. The first survived case of a patient with epistaxis and pituitary apoplexy due to ruptured aneurysm embedded within PA was reported and the literature was reviewed. A 53-year-old male patient presented to our institution with sudden onset epistaxis and progressive vision loss. Neurological examination revealed bilateral ptosis and dilated unresponsive pupils. A CT scan showed a large mass in the pituitary fossa with bony erosion. MRI revealed a large pituitary tumor and abnormal signal intensity in the tumor. No aneurysm was noted during the pre-operative MR angiography. Abundant arterial bleeding suddenly occurred during urgent transsphenoidal surgery. Digital subtraction angiography confirmed the presence of a 14 mm unexpected saccular aneurysm of right ICA in the cavernous sinus with the dome protruding into the sella turcica. Balloon test occlusion of the right ICA was undertaken and permanent occlusion was performed. The patient recovered well and received bromocriptine and thyroid hormone replacement therapy during the follow-up period. At 14-month followup, the patient had no neurological deficits, no features of ischaemia relating to the right ICA therapeutic occlusion. Our case indicated that epistaxis and pituitary apoplexy could be due to the rupture of an ICA aneurysm embedded in a PA. Clinical suspicion should remain high when evaluating any case of epistaxis and pituitary apoplexy. Optimal treatment should take into consideration individual features of the tumor, aneurysm, and patient. Making the correct diagnosis as well as identifying an appropriate management strategy is critical in the care of such patients.
Keywords: Cerebral aneurysm; epistaxis; pituitary adenoma; pituitary apoplexy.
Figures
Similar articles
-
Pituitary apoplexy caused by ruptured internal carotid artery aneurysm.Stroke. 2001 Feb;32(2):567-9. doi: 10.1161/01.str.32.2.567. Stroke. 2001. PMID: 11157198
-
A case of macroprolactinoma encasing an internal carotid artery aneurysm, presenting as pituitary apoplexy.Pituitary. 2008;11(3):307-11. doi: 10.1007/s11102-007-0063-5. Pituitary. 2008. PMID: 17899387
-
Simultaneous occurrence of subarachnoid hemorrhage and epistaxis due to ruptured petrous internal carotid artery aneurysm: association with transsphenoidal surgery and radiation therapy: case report.Neurol Med Chir (Tokyo). 2011;51(3):226-9. doi: 10.2176/nmc.51.226. Neurol Med Chir (Tokyo). 2011. PMID: 21441741
-
Pituitary adenoma apoplexy caused by rupture of an anterior communicating artery aneurysm: case report and literature review.World J Surg Oncol. 2015 Jul 30;13:228. doi: 10.1186/s12957-015-0653-z. World J Surg Oncol. 2015. PMID: 26220796 Free PMC article. Review.
-
Coexistence of aneurysmal subarachnoid hemorrhage and surgically identified pituitary apoplexy: a case report and review of the literature.J Med Case Rep. 2014 May 27;8:166. doi: 10.1186/1752-1947-8-166. J Med Case Rep. 2014. PMID: 24885333 Free PMC article. Review.
Cited by
-
Enlargement of an incidental internal carotid artery aneurysm embedded in pituitary adenoma associated with medical shrinkage of the tumor: Case report.Surg Neurol Int. 2018 Feb 14;9:30. doi: 10.4103/sni.sni_317_17. eCollection 2018. Surg Neurol Int. 2018. PMID: 29527388 Free PMC article.
-
Magnetic resonance imaging finding of coexistence of bilateral paraclinoid aneurysms in a patient with a nonfunctioning macroadenoma, simultaneous resection, and clipping: illustrative case.J Neurosurg Case Lessons. 2022 Mar 28;3(13):CASE21720. doi: 10.3171/CASE21720. Print 2022 Mar 28. J Neurosurg Case Lessons. 2022. PMID: 36273858 Free PMC article.
-
Giant Prolactinoma Embedded by Pseudoaneurysm of the Cavernous Carotid Artery Treated with a Tailored Therapeutic Scheme.J Neurosci Rural Pract. 2022 Jul 4;13(3):358-369. doi: 10.1055/s-0042-1749662. eCollection 2022 Jul. J Neurosci Rural Pract. 2022. PMID: 35945997 Free PMC article. Review.
-
Management of Coincident Pituitary Macroadenoma and Cavernous Carotid Aneurysm: A Systematic Literature Review.J Neurol Surg Rep. 2021 Sep 29;82(3):e25-e31. doi: 10.1055/s-0041-1735904. eCollection 2021 Jul. J Neurol Surg Rep. 2021. PMID: 34603930 Free PMC article.
-
The surgical management of pituitary apoplexy with occluded internal carotid artery and hidden intracranial aneurysm: illustrative case.J Neurosurg Case Lessons. 2021 Aug 2;2(5):CASE20115. doi: 10.3171/CASE20115. Print 2021 Aug 2. J Neurosurg Case Lessons. 2021. PMID: 36131582 Free PMC article.
References
-
- Oh MC, Kim EH, Kim SH. Coexistence of intracranial aneurysm in 800 patients with surgically confirmed pituitary adenoma. J Neurosurg. 2012;116:942–947. - PubMed
-
- Oshino S, Nishino A, Suzuki T, Arita H, Tateishi A, Matsumoto K, Shimokawa T, Kinoshita M, Yoshimine T, Saitoh Y. Prevalence of cerebral aneurysm in patients with acromegaly. Pituitary. 2013;16:195–201. - PubMed
-
- Sade B, Mohr G, Tampieri D, Rizzo A. Intrasellar aneurysm and a growth hormone-secreting pituitary macroadenoma. Case report. J Neurosurg. 2014;100:557–559. - PubMed
-
- Almeida Silva JM, Campos RR, Souza RR, Sette Dos Santos ME, Aguiar GB. Spontaneous subarachnoid haemorrhage from rupture of an anterior communicating artery aneurysm in a patient with pituitary macroadenoma. Neurocirugia (Astur) 2014;25:81–85. - PubMed
-
- Imamura J, Okuzono T, Okuzono Y. Fatal epistaxis caused by rupture of an intratumoral aneurysm enclosed by a large prolactinomacase report. Neurol Med Chir (Tokyo) 1998;38:654–656. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous