

Point-of-Care Multi-Organ Ultrasound Improves Diagnostic Accuracy in Adults Presenting to the Emergency Department with Acute Dyspnea
- PMID: 26823930
- PMCID: PMC4729418
- DOI: 10.5811/westjem.2015.11.28525
Point-of-Care Multi-Organ Ultrasound Improves Diagnostic Accuracy in Adults Presenting to the Emergency Department with Acute Dyspnea
Abstract
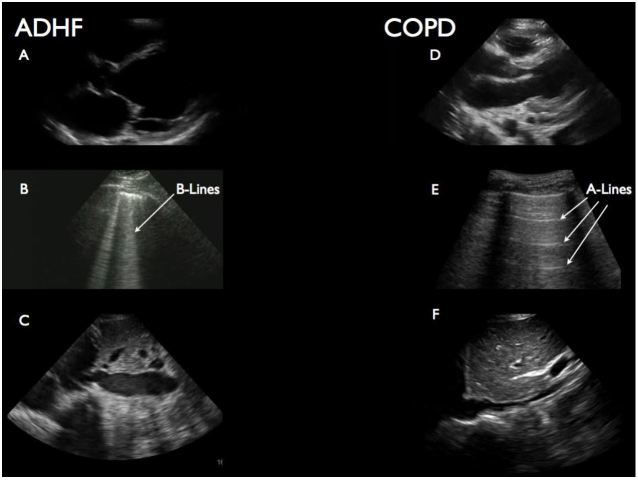
Introduction: Determining the etiology of acute dyspnea in emregency department (ED) patients is often difficult. Point-of-care ultrasound (POCUS) holds promise for improving immediate diagnostic accuracy (after history and physical), thus improving use of focused therapies. We evaluate the impact of a three-part POCUS exam, or "triple scan" (TS) - composed of abbreviated echocardiography, lung ultrasound and inferior vena cava (IVC) collapsibility assessment - on the treating physician's immediate diagnostic impression.
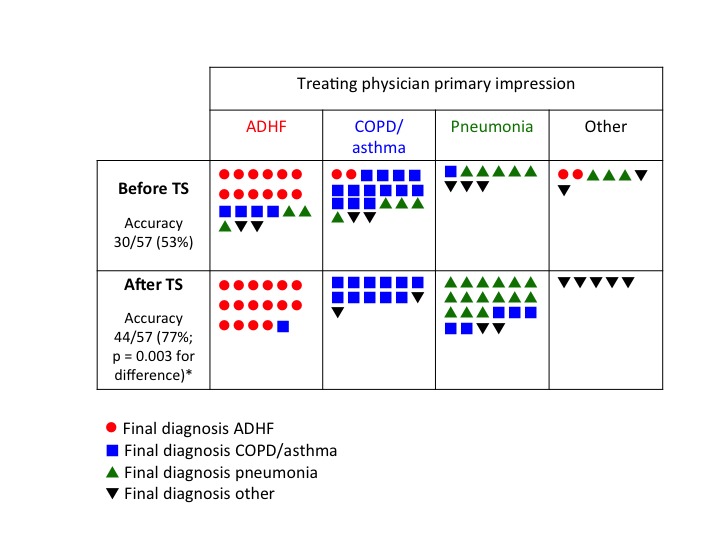
Methods: A convenience sample of adults presenting to our urban academic ED with acute dyspnea (Emergency Severity Index 1, 2) were prospectively enrolled when investigator sonographers were available. The method for performing components of the TS has been previously described in detail. Treating physicians rated the most likely diagnosis after history and physical but before other studies (except electrocardiogram) returned. An investigator then performed TS and disclosed the results, after which most likely diagnosis was reassessed. Final diagnosis (criterion standard) was based on medical record review by expert emergency medicine faculty blinded to TS result. We compared accuracy of pre-TS and post-TS impression (primary outcome) with McNemar's test. Test characteristics for treating physician impression were also calculated by dichotomizing acute decompensated heart failure (ADHF), chronic obstructive pulmonary disease (COPD) and pneumonia as present or absent.
Results: 57 patients were enrolled with the leading final diagnoses being ADHF (26%), COPD/asthma (30%), and pneumonia (28%). Overall accuracy of the treating physician's impression increased from 53% before TS to 77% after TS (p=0.003). The post-TS impression was 100% sensitive and 84% specific for ADHF.
Conclusion: In this small study, POCUS evaluation of the heart, lungs and IVC improved the treating physician's immediate overall diagnostic accuracy for ADHF, COPD/asthma and pneumonia and was particularly useful to immediately exclude ADHF as the cause of acute dyspnea.
Figures
Similar articles
-
Point-of-Care Ultrasonography for Evaluation of Acute Dyspnea in the ED.Chest. 2017 Jun;151(6):1295-1301. doi: 10.1016/j.chest.2017.02.003. Epub 2017 Feb 16. Chest. 2017. PMID: 28212836
-
Clinician-Performed Bedside Ultrasound in Improving Diagnostic Accuracy in Patients Presenting to the ED with Acute Dyspnea.West J Emerg Med. 2017 Apr;18(3):382-389. doi: 10.5811/westjem.2017.1.31223. Epub 2017 Mar 3. West J Emerg Med. 2017. PMID: 28435488 Free PMC article.
-
Assessment of left atrial size in addition to focused cardiopulmonary ultrasound improves diagnostic accuracy of acute heart failure in the Emergency Department.Echocardiography. 2018 Jun;35(6):785-791. doi: 10.1111/echo.13851. Epub 2018 Mar 9. Echocardiography. 2018. PMID: 29522655
-
Impact of ultrasound on management for dyspnea presentations in a Rwandan emergency department.Ultrasound J. 2019 Aug 20;11(1):18. doi: 10.1186/s13089-019-0133-8. Ultrasound J. 2019. PMID: 31432282 Free PMC article. Review.
-
Emergency department ultrasound for the detection of B-lines in the early diagnosis of acute decompensated heart failure: a systematic review and meta-analysis.CJEM. 2018 May;20(3):343-352. doi: 10.1017/cem.2018.27. Epub 2018 Apr 5. CJEM. 2018. PMID: 29619917
Cited by
-
Recommendations for Lung Ultrasound in Internal Medicine.Diagnostics (Basel). 2020 Aug 16;10(8):597. doi: 10.3390/diagnostics10080597. Diagnostics (Basel). 2020. PMID: 32824302 Free PMC article.
-
Point-of-care ultrasound modalities in terms of diagnosing acute decompensated heart failure in emergency department; a diagnostic accuracy study.Intern Emerg Med. 2020 Apr;15(3):491-499. doi: 10.1007/s11739-019-02233-x. Epub 2019 Nov 30. Intern Emerg Med. 2020. PMID: 31786750
-
Echoscopy in scanning cardiac diseases in critical care medicine.Med Klin Intensivmed Notfmed. 2023 May;118(4):293-300. doi: 10.1007/s00063-022-00935-3. Epub 2022 Jun 12. Med Klin Intensivmed Notfmed. 2023. PMID: 35691992 Clinical Trial. English.
-
Immunopathology, host-virus genome interactions, and effective vaccine development in SARS-CoV-2.Comput Struct Biotechnol J. 2020;18:3774-3787. doi: 10.1016/j.csbj.2020.11.011. Epub 2020 Nov 20. Comput Struct Biotechnol J. 2020. PMID: 33235690 Free PMC article. Review.
-
Effect of a Multiorgan Focused Clinical Ultrasonography on Length of Stay in Patients Admitted With a Cardiopulmonary Diagnosis: A Randomized Clinical Trial.JAMA Netw Open. 2021 Dec 1;4(12):e2138228. doi: 10.1001/jamanetworkopen.2021.38228. JAMA Netw Open. 2021. PMID: 34932107 Free PMC article. Clinical Trial.
References
-
- Knudsen CW, Omland T, Clopton P, et al. Diagnostic value of B-Type natriuretic peptide and chest radiographic findings in patients with acute dyspnea. Am J Med. 2004;116(6):363–8. - PubMed
-
- McCullough PA, Nowak RM, McCord J, et al. B-type natriuretic peptide and clinical judgment in emergency diagnosis of heart failure: analysis from Breathing Not Properly (BNP) Multinational Study. Circulation. 2002;106(4):416–22. - PubMed
-
- Wang CS, FitzGerald JM, Schulzer M, et al. Does this dyspneic patient in the emergency department have congestive heart failure? JAMA. 2005;294(15):1944–56. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
