

Posterior Cruciate Ligament Retention versus Posterior Stabilization for Total Knee Arthroplasty: A Meta-Analysis
- PMID: 26824368
- PMCID: PMC4732820
- DOI: 10.1371/journal.pone.0147865
Posterior Cruciate Ligament Retention versus Posterior Stabilization for Total Knee Arthroplasty: A Meta-Analysis
Abstract
Introduction: Although being debated for many years, the superiority of posterior cruciate-retaining (CR) total knee arthroplasty (TKA) and posterior-stabilized (PS) TKA remains controversial. We compare the knee scores, post-operative knee range of motion (ROM), radiological outcomes about knee kinematic and complications between CR TKA and PS TKA.
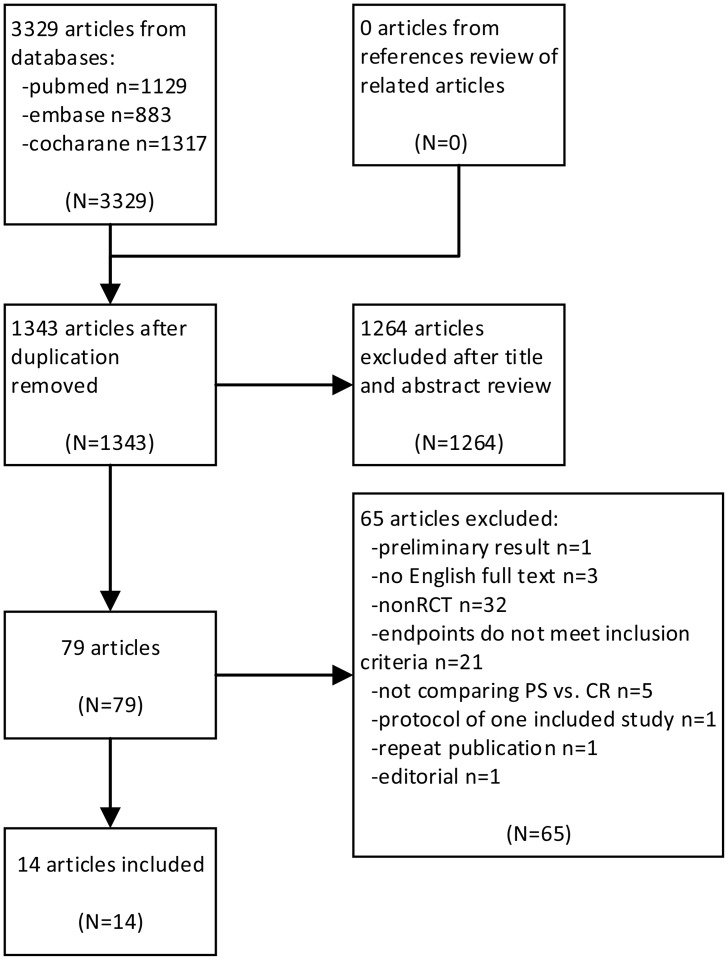
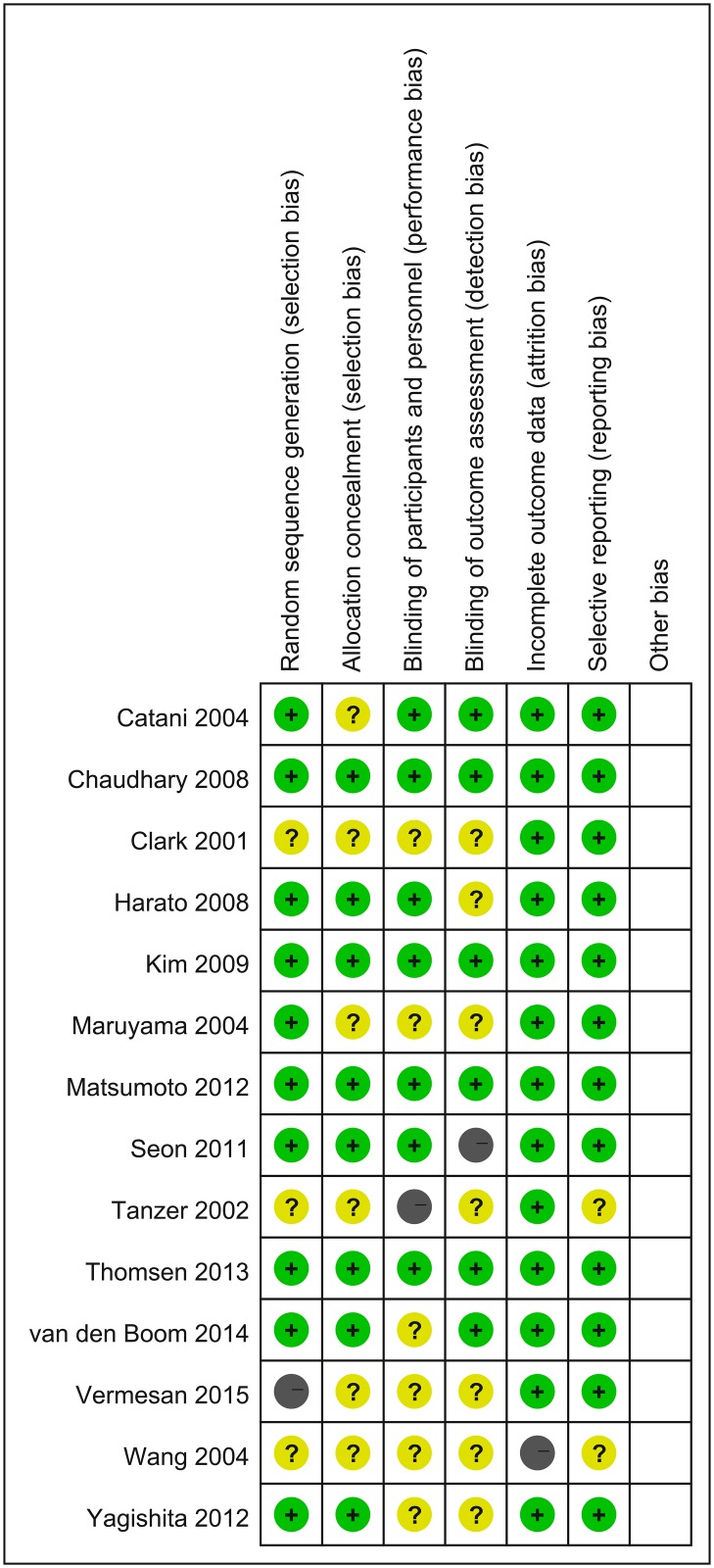
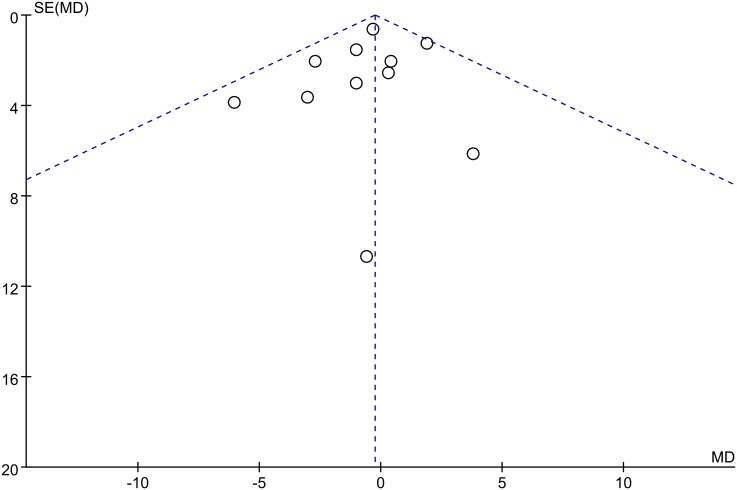
Methods: Literature published up to August 2015 was searched in PubMed, Embase and Cochrane databases, and meta-analysis was performed using the software, Review Manager version 5.3.
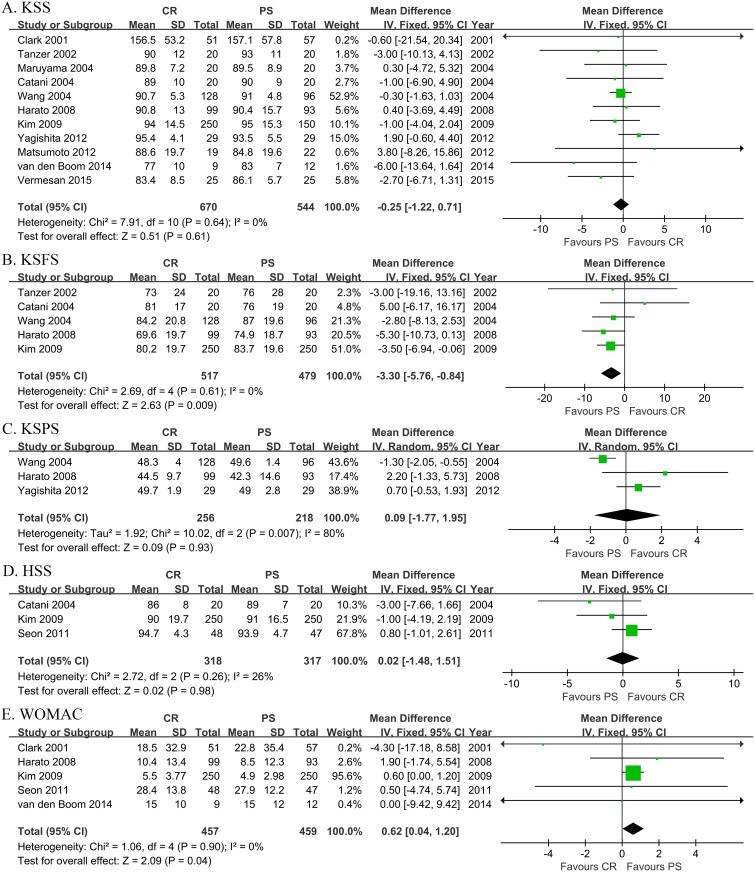
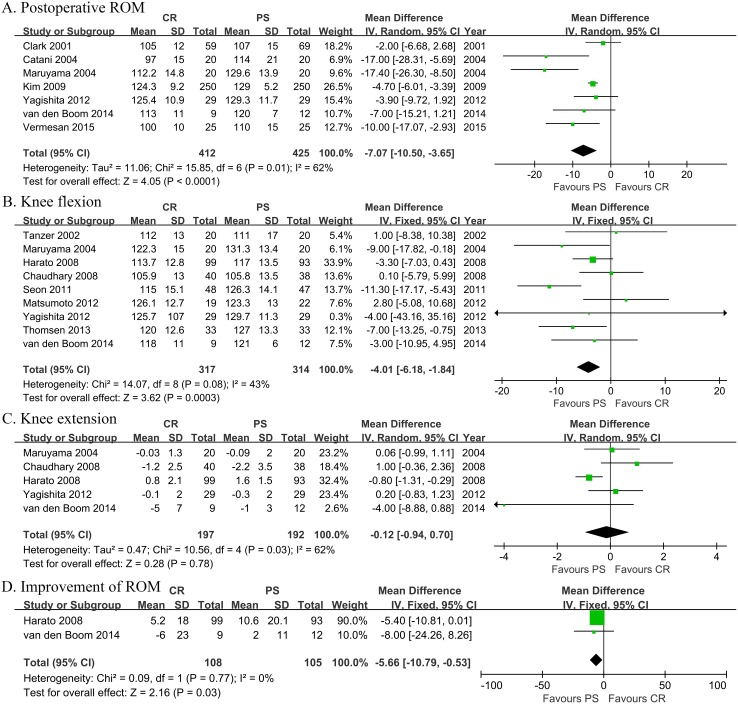
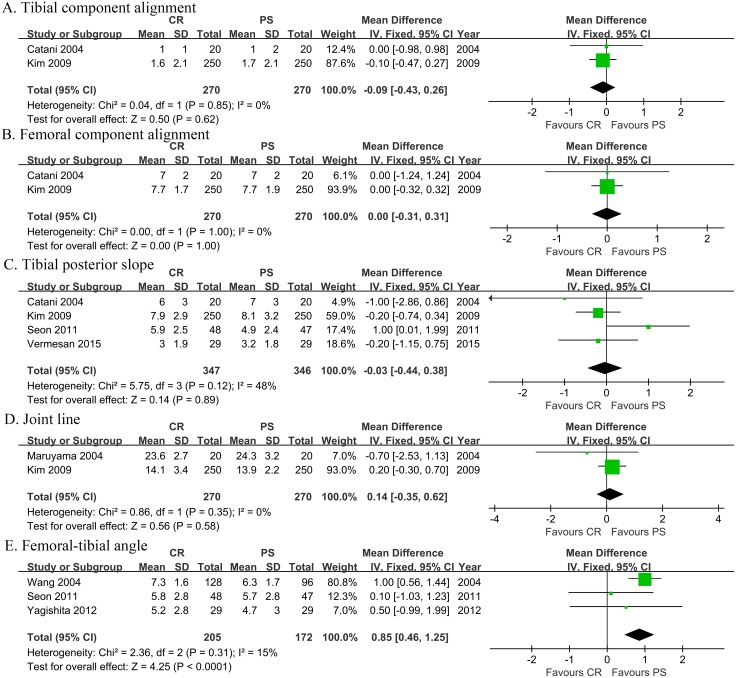
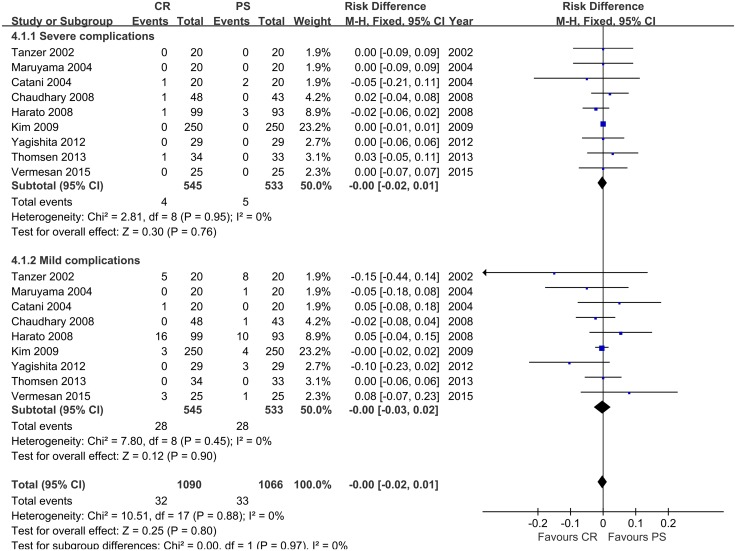
Results: Totally 14 random control trials (RCTs) on this topic were included for the analysis, which showed that PS and CR TKA had no significant difference in Knee Society knee Score (KSS), pain score (KSPS), Hospital for Special Surgery score (HSS), kinematic characteristics including postoperative component alignment, tibial posterior slope and joint line, and complication rate. However, PS TKA is superior to CR TKA regarding post-operative knee range of motion (ROM) [Random Effect model (RE), Mean Difference (MD) = -7.07, 95% Confidential Interval (CI) -10.50 to -3.65, p<0.0001], improvement of ROM (Fixed Effect model (FE), MD = -5.66, 95% CI -10.79 to -0.53, p = 0.03) and femoral-tibial angle [FE, MD = 0.85, 95% CI 0.46 to 1.25, p<0.0001].
Conclusions: There are no clinically relevant differences between CR and PS TKA in terms of clinical, functional, radiological outcome, and complications, while PS TKA is superior to CR TKA in respects of ROM, while whether this superiority matters or not in clinical practice still needs further investigation and longer follow-up.
Conflict of interest statement
Figures
Similar articles
-
Effect of posterior-stabilized and cruciate-retaining implants on three-dimensional kinematic characteristics after total knee arthroplasty.Jt Dis Relat Surg. 2025 Jan 2;36(1):3-14. doi: 10.52312/jdrs.2024.1836. Epub 2024 Nov 5. Jt Dis Relat Surg. 2025. PMID: 39719896 Free PMC article.
-
[A comparative analysis of the efficacy of Advance(®) medial pivot prosthesis knee arthroplasty with posterior cruciate ligament retention or substituting based on propensity score matching].Zhonghua Yi Xue Za Zhi. 2020 Jan 21;100(3):187-191. doi: 10.3760/cma.j.issn.0376-2491.2020.03.006. Zhonghua Yi Xue Za Zhi. 2020. PMID: 32008284 Chinese.
-
Anteroposterior translation and range of motion after total knee arthroplasty using posterior cruciate ligament-retaining versus posterior cruciate ligament-substituting prostheses.Knee Surg Sports Traumatol Arthrosc. 2017 Nov;25(11):3536-3542. doi: 10.1007/s00167-016-4257-0. Epub 2016 Aug 2. Knee Surg Sports Traumatol Arthrosc. 2017. PMID: 27485124
-
Posterior cruciate-retaining versus posterior stabilized total knee arthroplasty: a meta-analysis of randomized controlled trials.Knee Surg Sports Traumatol Arthrosc. 2014 Mar;22(3):556-64. doi: 10.1007/s00167-012-2275-0. Epub 2012 Nov 3. Knee Surg Sports Traumatol Arthrosc. 2014. PMID: 23117166 Review.
-
Comparison of posterior cruciate retention and substitution in total knee arthroplasty during gait: a systematic review and meta-analysis.J Orthop Surg Res. 2022 Mar 9;17(1):152. doi: 10.1186/s13018-022-03047-y. J Orthop Surg Res. 2022. PMID: 35264236 Free PMC article.
Cited by
-
Predicting clinical outcomes after total knee arthroplasty from preoperative radiographic factors of the knee osteoarthritis.BMC Musculoskelet Disord. 2020 Jan 6;21(1):9. doi: 10.1186/s12891-019-3029-7. BMC Musculoskelet Disord. 2020. PMID: 31906935 Free PMC article.
-
Comparable joint awareness and implant survival at midterm follow-up between CR and PS TKA: An anatomic phenotype-based propensity score-matched analysis.J Exp Orthop. 2025 May 19;12(2):e70242. doi: 10.1002/jeo2.70242. eCollection 2025 Apr. J Exp Orthop. 2025. PMID: 40390854 Free PMC article.
-
Cruciate-Retaining Implants Do Not Provide a More Natural Joint Feeling Than Cruciate-Substituting Implants in Total Knee Arthroplasty: A Systematic Review and Meta-Analysis.JB JS Open Access. 2025 Aug 7;10(3):e25.00136. doi: 10.2106/JBJS.OA.25.00136. eCollection 2025 Jul-Sep. JB JS Open Access. 2025. PMID: 40777211 Free PMC article. Review.
-
Effect of posterior-stabilized and cruciate-retaining implants on three-dimensional kinematic characteristics after total knee arthroplasty.Jt Dis Relat Surg. 2025 Jan 2;36(1):3-14. doi: 10.52312/jdrs.2024.1836. Epub 2024 Nov 5. Jt Dis Relat Surg. 2025. PMID: 39719896 Free PMC article.
-
A Novel Technique for Restricted Kinematic Alignment Total Knee Arthroplasty Without Computer-Assisted Devices.Cureus. 2024 Aug 19;16(8):e67233. doi: 10.7759/cureus.67233. eCollection 2024 Aug. Cureus. 2024. PMID: 39301339 Free PMC article.
References
-
- Swanik CB, Lephart SM, Rubash HE. Proprioception, kinesthesia, and balance after total knee arthroplasty with cruciate-retaining and posterior stabilized prostheses. J Bone Joint Surg Am. 2004; 86-A: 328–334. - PubMed
-
- Harato K, Bourne RB, Victor J, Snyder M, Hart J, Ries MD. Midterm comparison of posterior cruciate-retaining versus -substituting total knee arthroplasty using the Genesis II prosthesis. A multicenter prospective randomized clinical trial. Knee. 2008; 15: 217–221. 10.1016/j.knee.2007.12.007 - DOI - PubMed
-
- Conditt MA, Noble PC, Bertolusso R, Woody J, Parsley BS. The PCL significantly affects the functional outcome of total knee arthroplasty. J Arthroplast. 2004;19(7 suppl 2):107–112. - PubMed
-
- Straw R, Kulkarni S, Attfield S, Wilton TJ. Posterior cruciate ligament at total knee replacement. Essential, beneficial or a hindrance? J Bone Jt Surg [Br]. 2003;85B: 671–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
