

Current Staging Procedures in Urinary Bladder Cancer
- PMID: 26824925
- PMCID: PMC4665464
- DOI: 10.3390/diagnostics3030315
Current Staging Procedures in Urinary Bladder Cancer
Abstract
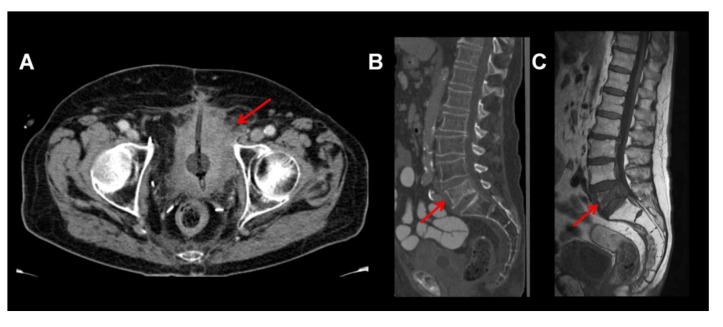
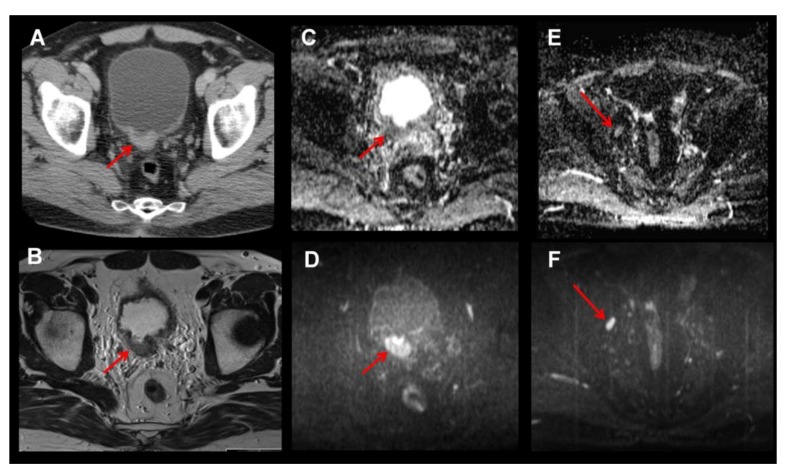
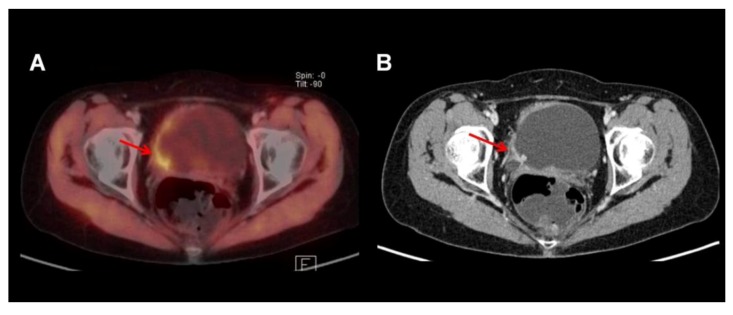
Currently computed tomography (CT) represents the most widely used standard imaging modality in muscle-invasive urinary bladder cancer. Visualization of local tumor or depth of invasion as well as lymph node staging, however, is often impaired. Magnetic resonance imaging (MRI) with diffusion-weighted sequences, determination of apparent diffusion coefficient (ADC) values or utilization of superparamagnetic iron nanoparticles potentially exhibits advantages in the assessment of local tumor or lymph node involvement and therefore might play a role in routine staging of urinary bladder cancer in the future. Likewise, positron emission tomography (PET) with the currently utilized tracers (18)F-FDG, (11)C-choline and (11)C-acetate is investigated in bladder cancer patients-mostly in combination with diagnostic CT. Although promising results could be obtained for these PET/CT examinations in smaller series, their true value cannot be determined at present.
Keywords: FDG; MRI; PET/CT; actetate; choline; urinary bladder cancer.
Figures
Similar articles
-
[Functional imaging in bladder cancer].Urologe A. 2013 Apr;52(4):509-14. doi: 10.1007/s00120-012-3097-x. Urologe A. 2013. PMID: 23483270 German.
-
More advantages in detecting bone and soft tissue metastases from prostate cancer using 18F-PSMA PET/CT.Hell J Nucl Med. 2019 Jan-Apr;22(1):6-9. doi: 10.1967/s002449910952. Epub 2019 Mar 7. Hell J Nucl Med. 2019. PMID: 30843003
-
Preoperative lymph-node staging of invasive urothelial bladder cancer with 18F-fluorodeoxyglucose positron emission tomography/computed axial tomography and magnetic resonance imaging: correlation with histopathology.Scand J Urol Nephrol. 2011 Mar;45(2):122-8. doi: 10.3109/00365599.2010.544672. Epub 2011 Jan 13. Scand J Urol Nephrol. 2011. PMID: 21231796
-
Positron emission tomography for prostate, bladder, and renal cancer.Semin Nucl Med. 2004 Oct;34(4):274-92. doi: 10.1053/j.semnuclmed.2004.06.004. Semin Nucl Med. 2004. PMID: 15493005 Review.
-
Update on novel imaging techniques for the detection of lymph node metastases in bladder cancer.Minerva Urol Nefrol. 2016 Apr;68(2):138-49. Minerva Urol Nefrol. 2016. PMID: 27271230 Review.
Cited by
-
Predictive Value of Computed Tomography Following Neoadjuvant Chemotherapy for Muscle Invasive Bladder Cancer.Bladder Cancer. 2023 Jun 27;9(2):167-174. doi: 10.3233/BLC-230015. eCollection 2023. Bladder Cancer. 2023. PMID: 38993298 Free PMC article.
-
Computed-tomography based scoring system predicts outcome for clinical lymph node-positive patients undergoing radical cystectomy.Int Braz J Urol. 2022 Jan-Feb;48(1):89-98. doi: 10.1590/S1677-5538.IBJU.2021.0329. Int Braz J Urol. 2022. PMID: 34528776 Free PMC article.
-
Targeting IL-5Rα with antibody-conjugates reveals a strategy for imaging and therapy for invasive bladder cancer.Oncoimmunology. 2017 May 19;6(10):e1331195. doi: 10.1080/2162402X.2017.1331195. eCollection 2017. Oncoimmunology. 2017. PMID: 29123949 Free PMC article.
-
Utility of early dynamic and delayed post-diuretic 18F-FDG PET/CT SUVmax in predicting tumour grade and T-stage of urinary bladder carcinoma: results from a prospective single centre study.Br J Radiol. 2017 Apr;90(1072):20160787. doi: 10.1259/bjr.20160787. Epub 2017 Mar 3. Br J Radiol. 2017. PMID: 28256904 Free PMC article.
-
Recurrent bladder carcinoma: clinical and prognostic role of 18 F-FDG PET/CT.Eur J Nucl Med Mol Imaging. 2017 Feb;44(2):224-233. doi: 10.1007/s00259-016-3500-8. Epub 2016 Aug 26. Eur J Nucl Med Mol Imaging. 2017. PMID: 27565154
References
-
- Stenzl A., Witjes J.A., Cowan N.C., De Santis M., Kuczyk M., Lebret T., Merseburger A.S., Ribal M.J., Sherif A. Guidelines on Bladder Cancer Muscle-Invasive and Metastatic. [(accessed on 17 May 2013)]. Available online: http://www.uroweb.org/gls/pdf/07_%20Bladder%20Cancer.pdf.
-
- Shariat S.F., Ehdaie B., Rink M., Cha E.K., Svatek R.S., Chromecki T.F., Fajkovic H., Novara G., David S.G., Daneshmand S., et al. Clinical nodal staging scores for bladder cancer: A proposal for preoperative risk assessment. Eur. Urol. 2012;61:237–242. doi: 10.1016/j.eururo.2011.10.011. - DOI - PubMed
-
- Grossman H.B., Natale R.B., Tangen C.M., Speights V.O., Vogelzang N.J., Trump D.L., deVere White R.W., Sarosdy M.F., Wood D.P., Jr., Raghavan D., et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N. Engl. J. Med. 2003;349:859–866. doi: 10.1056/NEJMoa022148. - DOI - PubMed
-
- Vale C., Advanced-Bladder-Cancer-Meta-Analysis-Collaboration Neoadjuvant chemotherapy in invasive bladder cancer: A systematic review and meta-analysis. Lancet. 2003;361:1927–1934. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
