

Population Care Management and Team-Based Approach to Reduce Racial Disparities among African Americans/Blacks with Hypertension
- PMID: 26824963
- PMCID: PMC4732795
- DOI: 10.7812/TPP/15-052
Population Care Management and Team-Based Approach to Reduce Racial Disparities among African Americans/Blacks with Hypertension
Abstract
Objectives: At Kaiser Permanente, national Equitable Care Health Outcomes (ECHO) Reports with a baseline measurement of 16 Healthcare Effectiveness Data and Information Set measures stratified by race and ethnicity showed a disparity of 8.1 percentage points in blood pressure (BP) control rates between African- American/black (black) and white members. The aims of this study were to describe a population care management team-based approach to improve BP control for large populations and to explain how a culturally tailored, patient-centered approach can address this racial disparity.
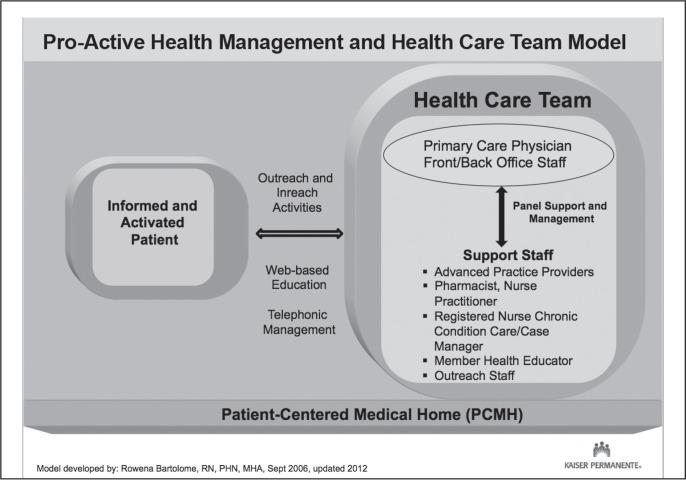
Methods: These strategies were implemented through: 1) physician-led educational programs on treatment intensification, medication adherence, and consistent use of clinical practice guidelines; 2) building strong care teams by defining individual roles and responsibilities in hypertension management; 3) redesign of the care delivery system to expand access; and 4) programs on culturally tailored communication tools and self-management.
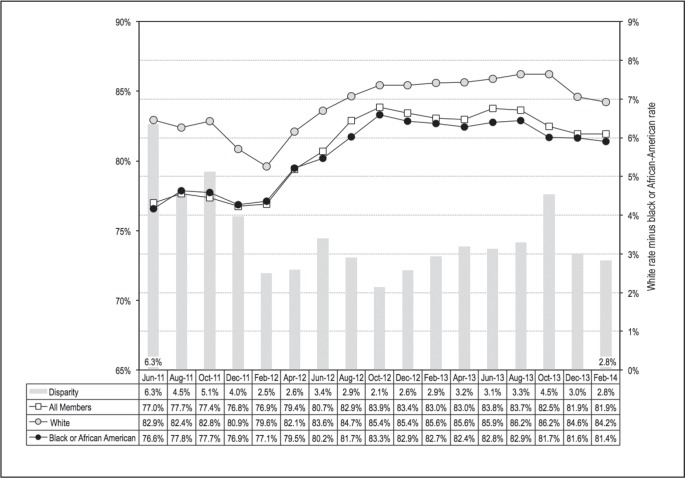
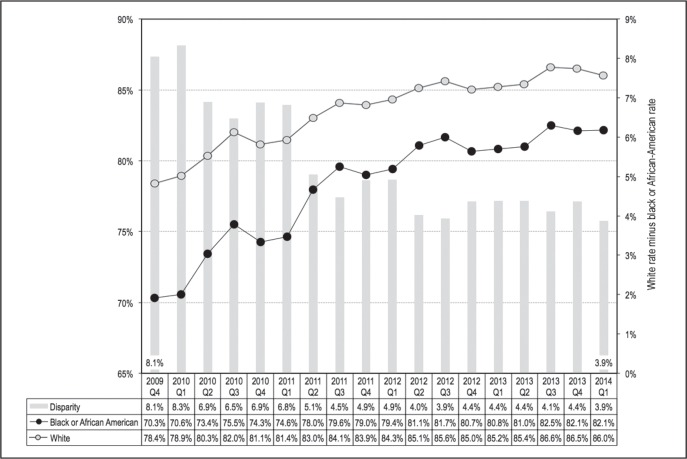
Results: At a physician practice level where 65% of patients with hypertension were black, BP control rates (< 140/90 mmHg) for blacks improved from 76.6% to 81.4%, and control rates for whites increased from 82.9% to 84.2%. The racial gap narrowed from 6.3% to 2.8%. As these successful practices continue to spread throughout the program, the health disparity gap in BP control has decreased by 50%, from 8.1% to 3.9%.
Conclusion: A sustainable program to collect self-reported race, ethnicity, and language preference data integrated with successful population care management programs provided the foundation for addressing health disparities. Cultural tailoring of a multilevel team-based approach closed the gap for blacks with hypertension.
Figures
Similar articles
-
Effect of a Coordinated Community and Chronic Care Model Team Intervention vs Usual Care on Systolic Blood Pressure in Patients With Stroke or Transient Ischemic Attack: The SUCCEED Randomized Clinical Trial.JAMA Netw Open. 2021 Feb 1;4(2):e2036227. doi: 10.1001/jamanetworkopen.2020.36227. JAMA Netw Open. 2021. PMID: 33587132 Free PMC article. Clinical Trial.
-
Adapting and Evaluating a Health System Intervention From Kaiser Permanente to Improve Hypertension Management and Control in a Large Network of Safety-Net Clinics.Circ Cardiovasc Qual Outcomes. 2018 Jul;11(7):e004386. doi: 10.1161/CIRCOUTCOMES.117.004386. Circ Cardiovasc Qual Outcomes. 2018. PMID: 30002140 Free PMC article.
-
Understanding racial disparities in treatment intensification for hypertension management.J Gen Intern Med. 2010 Aug;25(8):819-25. doi: 10.1007/s11606-010-1342-9. Epub 2010 Apr 13. J Gen Intern Med. 2010. PMID: 20386998 Free PMC article.
-
Hypertension in African Americans.Curr Cardiol Rep. 2017 Oct 28;19(12):129. doi: 10.1007/s11886-017-0933-z. Curr Cardiol Rep. 2017. PMID: 29081008 Review.
-
Hypertension Treatment in Blacks: Discussion of the U.S. Clinical Practice Guidelines.Prog Cardiovasc Dis. 2016 Nov-Dec;59(3):282-288. doi: 10.1016/j.pcad.2016.09.004. Epub 2016 Sep 29. Prog Cardiovasc Dis. 2016. PMID: 27693861 Free PMC article. Review.
Cited by
-
Post-acute sequelae of SARS-CoV-2 with clinical condition definitions and comparison in a matched cohort.Nat Commun. 2022 Oct 12;13(1):5822. doi: 10.1038/s41467-022-33573-6. Nat Commun. 2022. PMID: 36224218 Free PMC article.
-
Emergency Department Utilization, Hospital Admissions, and Office-Based Physician Visits Among Under-Resourced African American and Latino Older Adults.J Racial Ethn Health Disparities. 2023 Feb;10(1):205-218. doi: 10.1007/s40615-021-01211-4. Epub 2022 Jan 10. J Racial Ethn Health Disparities. 2023. PMID: 35006585 Free PMC article.
-
Leveraging Implementation Science for Cardiovascular Health Equity: A Scientific Statement From the American Heart Association.Circulation. 2022 Nov 8;146(19):e260-e278. doi: 10.1161/CIR.0000000000001096. Epub 2022 Oct 10. Circulation. 2022. PMID: 36214131 Free PMC article. Review.
-
Clinical Multiteam System Composition and Complexity Among Newly Diagnosed Early-Stage Breast, Colorectal, and Lung Cancer Patients With Multiple Chronic Conditions: A SEER-Medicare Analysis.JCO Oncol Pract. 2023 Jan;19(1):e33-e42. doi: 10.1200/OP.22.00304. Epub 2022 Dec 6. JCO Oncol Pract. 2023. PMID: 36473151 Free PMC article.
-
An Equity Agenda for the Field of Health Care Quality Improvement.NAM Perspect. 2021 Sep 15;2021:10.31478/202109b. doi: 10.31478/202109b. eCollection 2021. NAM Perspect. 2021. PMID: 34901779 Free PMC article. Review. No abstract available.
References
-
- Centers for Disease Control and Prevention (CDC) Vital signs: awareness and treatment of uncontrolled hypertension among adults—United States, 2003–2010. MMWR Morb Mortal Wkly Rep. 2012 Sep 7;61:703–9. - PubMed
-
- Heidenreich PA, Trogdon JG, Khavjou OA, et al. American Heart Association Advocacy Coordinating Committee. Stroke Council. Council on Cardiovascular Radiology and Intervention Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011 Mar 1;123(8):933–44. DOI: http://dx.doi.org/10.1161/CIR.0b013e31820a55f5. - DOI - PubMed
-
- Nwankwo T, Yoon SS, Burt V, Gu Q. Hypertension among adults in the United States: National Health and Nutrition Examination Survey, 2011–2012. NCHS Data Brief. 2013 Oct;(133):1–8. - PubMed
-
- Yoon PW, Gillespie CD, George MG, Wall HK, Centers for Disease Control and Prevention (CDC) Control of hypertension among adults— National Health and Nutrition Examination Survey, United States, 2005–2008. MMWR Morb Mortal Wkly Rep. 2012 Jun 15;61(Suppl):19–25. - PubMed
-
- Go AS, Mozaffarian D, Roger VL, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics—2014 update: a report from the American Heart Association. Circulation. 2014 Jan 21;129(3):e28–e292. DOI: http://dx.doi.org/10.1161/01.cir.0000441139.02102.80. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
