

Use of Intensive Care Services for Medicare Beneficiaries Undergoing Major Surgical Procedures
- PMID: 26825149
- PMCID: PMC4792707
- DOI: 10.1097/ALN.0000000000001024
Use of Intensive Care Services for Medicare Beneficiaries Undergoing Major Surgical Procedures
Abstract
Background: Use of intensive care after major surgical procedures and whether routinely admitting patients to intensive care units (ICUs) improve outcomes or increase costs is unknown.
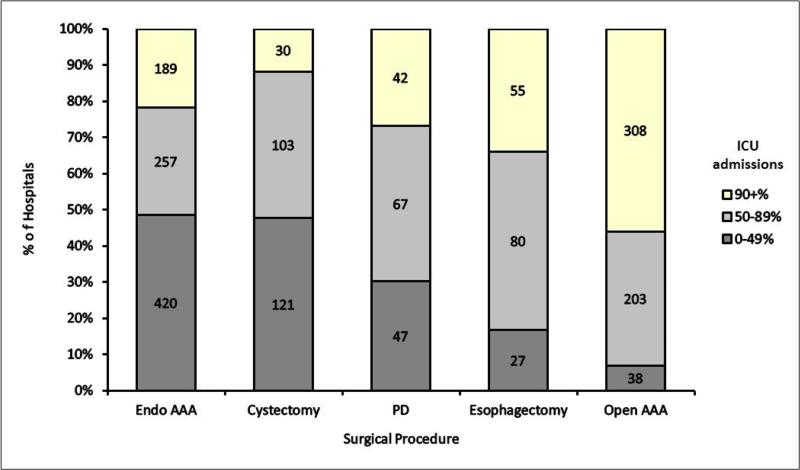
Methods: The authors examined frequency of admission to an ICU during the hospital stay for Medicare beneficiaries undergoing selected major surgical procedures: elective endovascular abdominal aortic aneurysm (AAA) repair, cystectomy, pancreaticoduodenectomy, esophagectomy, and elective open AAA repair. The authors compared hospital mortality, length of stay, and Medicare payments for patients receiving each procedure in hospitals admitting patients to the ICU less than 50% of the time (low use), 50 to 89% (moderate use), and 90% or greater (high use), adjusting for patient and hospital factors.
Results: The cohort ranged from 7,878 patients in 162 hospitals for esophagectomies to 69,989 patients in 866 hospitals for endovascular AAA. Overall admission to ICU ranged from 35.6% (endovascular AAA) to 71.3% (open AAA). Admission to ICU across hospitals ranged from less than 5% to 100% of patients for each surgical procedure. There was no association between hospital use of intensive care and mortality for any of the five surgical procedures. There was a consistent association between high use of intensive care with longer length of hospital stay and higher Medicare payments only for endovascular AAA.
Conclusions: There is little consensus regarding the need for intensive care for patients undergoing major surgical procedures and no relationship between a hospital's use of intensive care and hospital mortality. There is also no consistent relationship across surgical procedures between use of intensive care and either length of hospital stay or payments for care.
Figures
Comment in
-
Intensive Care after High-risk Surgery: What's in a Name?Anesthesiology. 2016 Apr;124(4):761-2. doi: 10.1097/ALN.0000000000001025. Anesthesiology. 2016. PMID: 26825150 No abstract available.
References
-
- Bainbridge D, Martin J, Arango M, Cheng D. Perioperative and anaesthetic-related mortality in developed and developing countries: a systematic review and meta-analysis. Lancet. 2012;380:1075–81. - PubMed
-
- Avidan MS, Kheterpal S. Perioperative mortality in developed and developing countries. Lancet. 2012;380:1038–9. - PubMed
-
- Robert R, Reignier J, Tournoux-Facon C, Boulain T, Lesieur O, Gissot V, Souday V, Hamrouni M, Chapon C, Gouello JP. Refusal of ICU Admission Due to a Full Unit: Impact on Mortality. Am J Respir Crit Care Med. 2012;185:1081–1087. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
