

Prehospital Blood Product Resuscitation for Trauma: A Systematic Review
- PMID: 26825635
- PMCID: PMC4933578
- DOI: 10.1097/SHK.0000000000000569
Prehospital Blood Product Resuscitation for Trauma: A Systematic Review
Abstract
Introduction: Administration of high ratios of plasma to packed red blood cells is a routine practice for in-hospital trauma resuscitation. Military and civilian emergency teams are increasingly carrying prehospital blood products (PHBP) for trauma resuscitation. This study systematically reviewed the clinical literature to determine the extent to which the available evidence supports this practice.
Methods: Bibliographic databases and other sources were searched to July 2015 using keywords and index terms related to the intervention, setting, and condition. Standard systematic review methodology aimed at minimizing bias was used for study selection, data extraction, and quality assessment (protocol registration
Prospero: CRD42014013794). Synthesis was mainly narrative with random effects model meta-analysis limited to mortality outcomes.
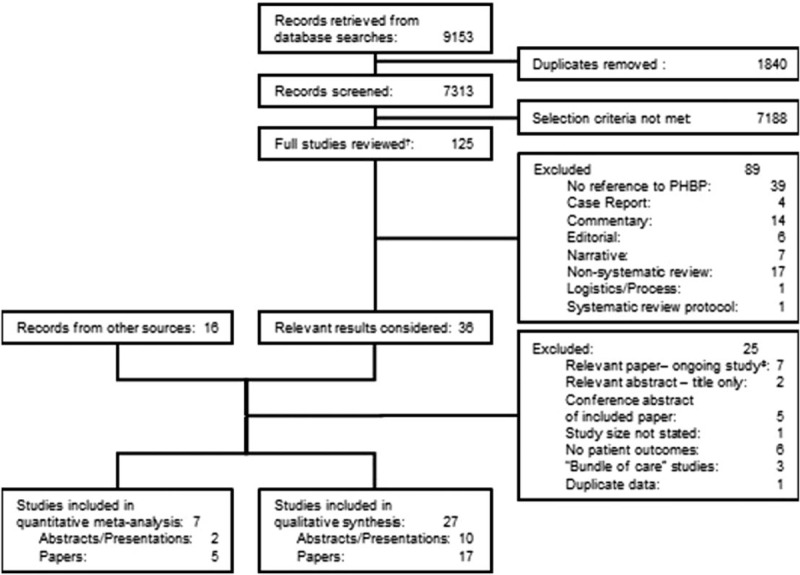
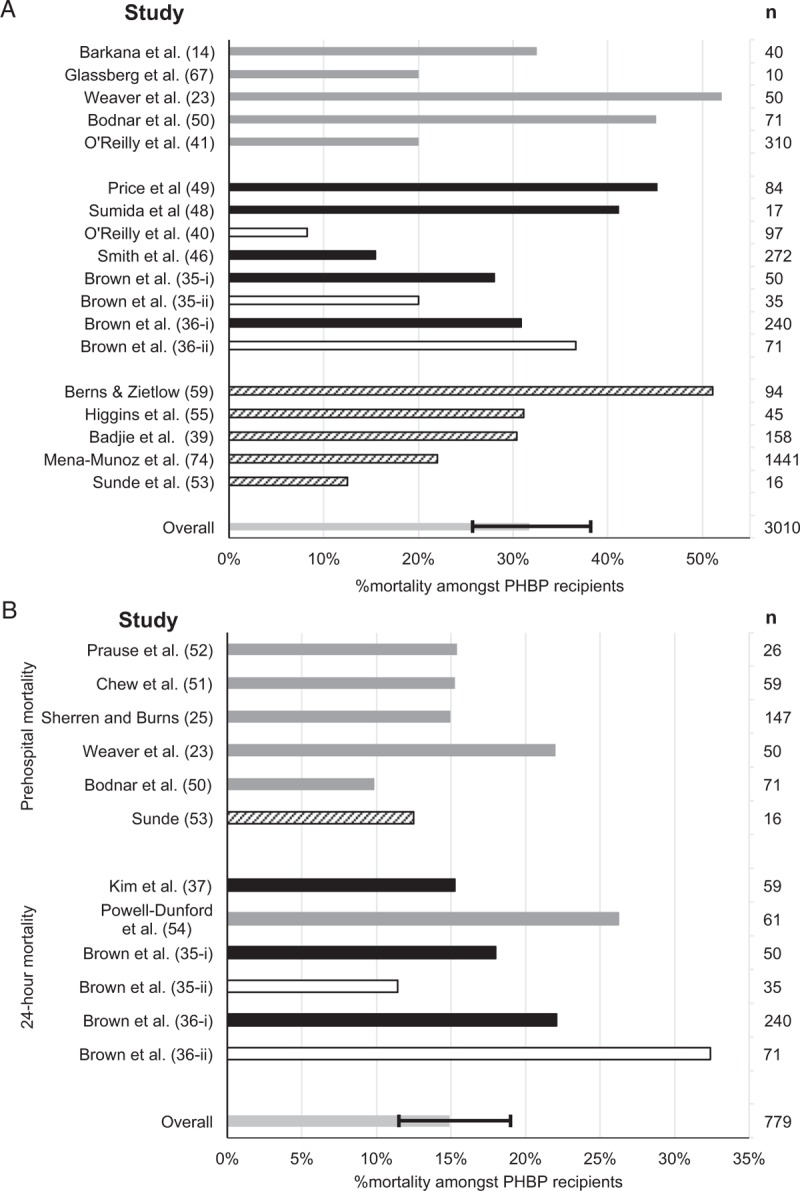
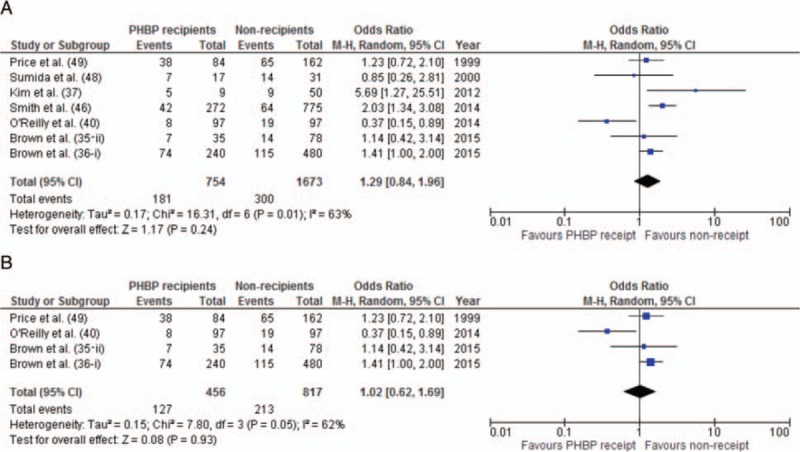
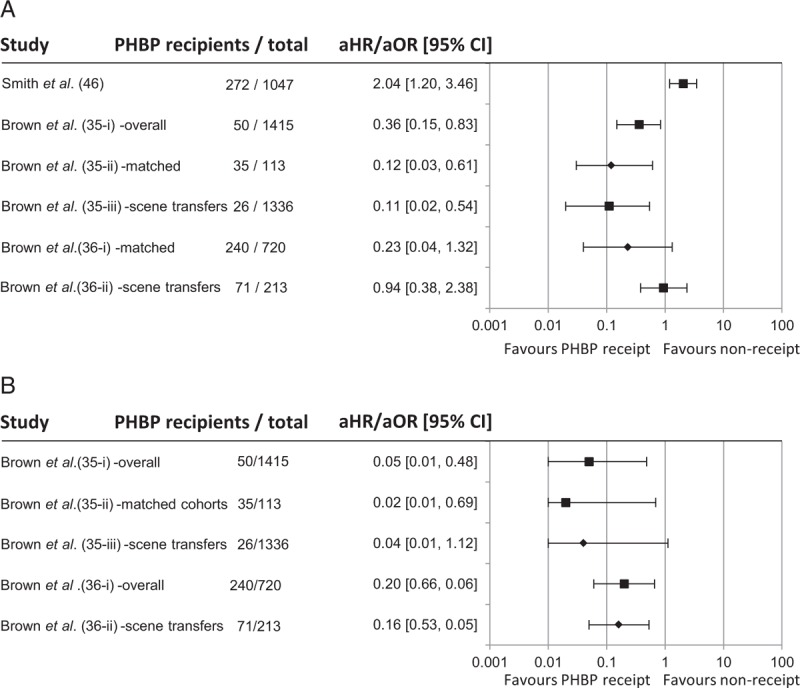
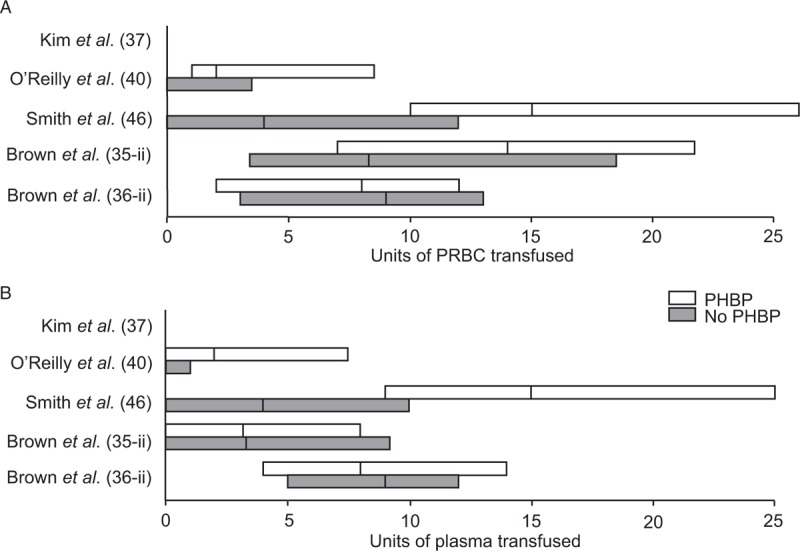
Results: No prospective comparative or randomized studies were identified. Sixteen case series and 11 comparative studies were included in the review. Seven studies included mixed populations of trauma and non-trauma patients. Twenty-five of 27 studies provided only very low quality evidence. No association between PHBP and survival was found (OR for mortality: 1.29, 95% CI: 0.84-1.96, P = 0.24). A single study showed improved survival in the first 24 h. No consistent physiological or biochemical benefit was identified, nor was there evidence of reduced in-hospital transfusion requirements. Transfusion reactions were rare, suggesting the short-term safety of PHBP administration.
Conclusions: While PHBP resuscitation appears logical, the clinical literature is limited, provides only poor quality evidence, and does not demonstrate improved outcomes. No conclusions as to efficacy can be drawn. The results of randomized controlled trials are awaited.
Conflict of interest statement
1“Military”: casualties of armed conflict.
FDP indicates Freeze Dried Plasma; mISS and mNISS, ISS and NISS derived from the military edition of the Abbreviated Injury Scale (2005).
Figures
References
-
- Bailey JA, Morrison JJ, Rasmussen TE. Military trauma system in Afghanistan: lessons for civil systems? Curr Opin Crit Care 2013; 19 6:569–577. - PubMed
-
- Penn-Barwell JG, Roberts SA, Midwinter MJ, Bishop JR. Improved survival in UK combat casualties from Iraq and Afghanistan: 2003-2012. J Trauma Acute Care Surg 2015; 78 5:1014–1020. - PubMed
-
- Dawes R, Thomas GO. Battlefield resuscitation. Curr Opin Crit Care 2009; 15 6:527–535. - PubMed
-
- Bhangu A, Nepogodiev D, Doughty H, Bowley DM. Meta-analysis of plasma to red blood cell ratios and mortality in massive blood transfusions for trauma. Injury 2013; 44 12:1693–1699. - PubMed
-
- Murad MH, Stubbs JR, Gandhi MJ, Wang AT, Paul A, Erwin PJ, Montori VM, Roback JD. The effect of plasma transfusion on morbidity and mortality: a systematic review and meta-analysis. Transfusion 2010; 50 6:1370–1383. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
