

Janus kinase inhibition lessens inflammation and ameliorates disease in murine models of hemophagocytic lymphohistiocytosis
- PMID: 26825707
- PMCID: PMC4817310
- DOI: 10.1182/blood-2015-12-684399
Janus kinase inhibition lessens inflammation and ameliorates disease in murine models of hemophagocytic lymphohistiocytosis
Abstract
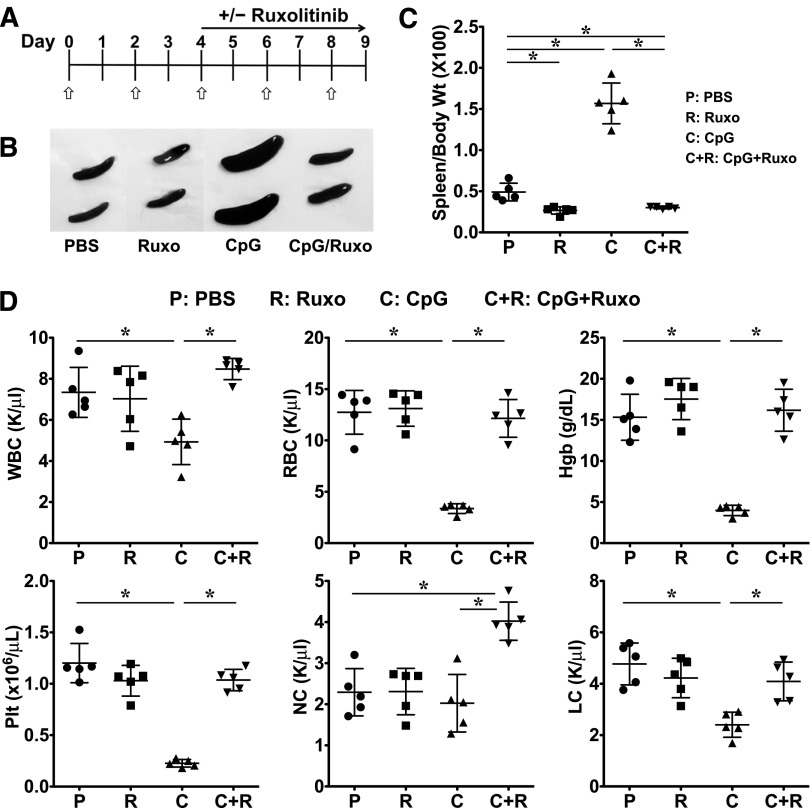
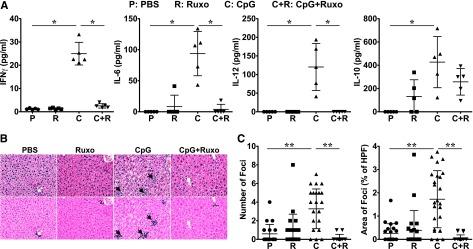
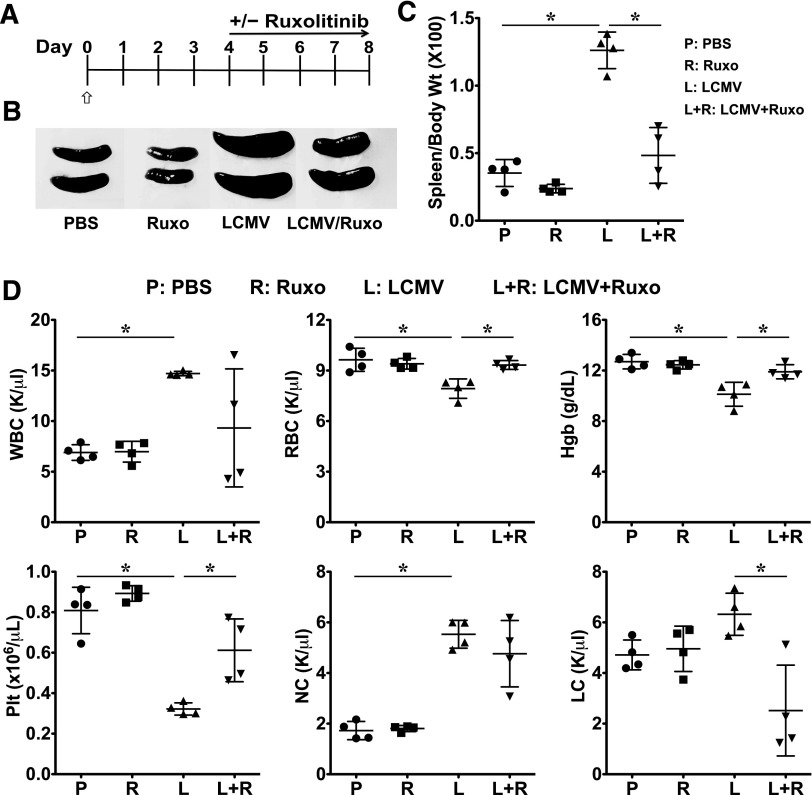
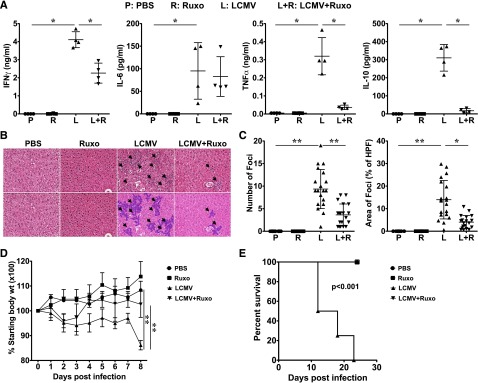
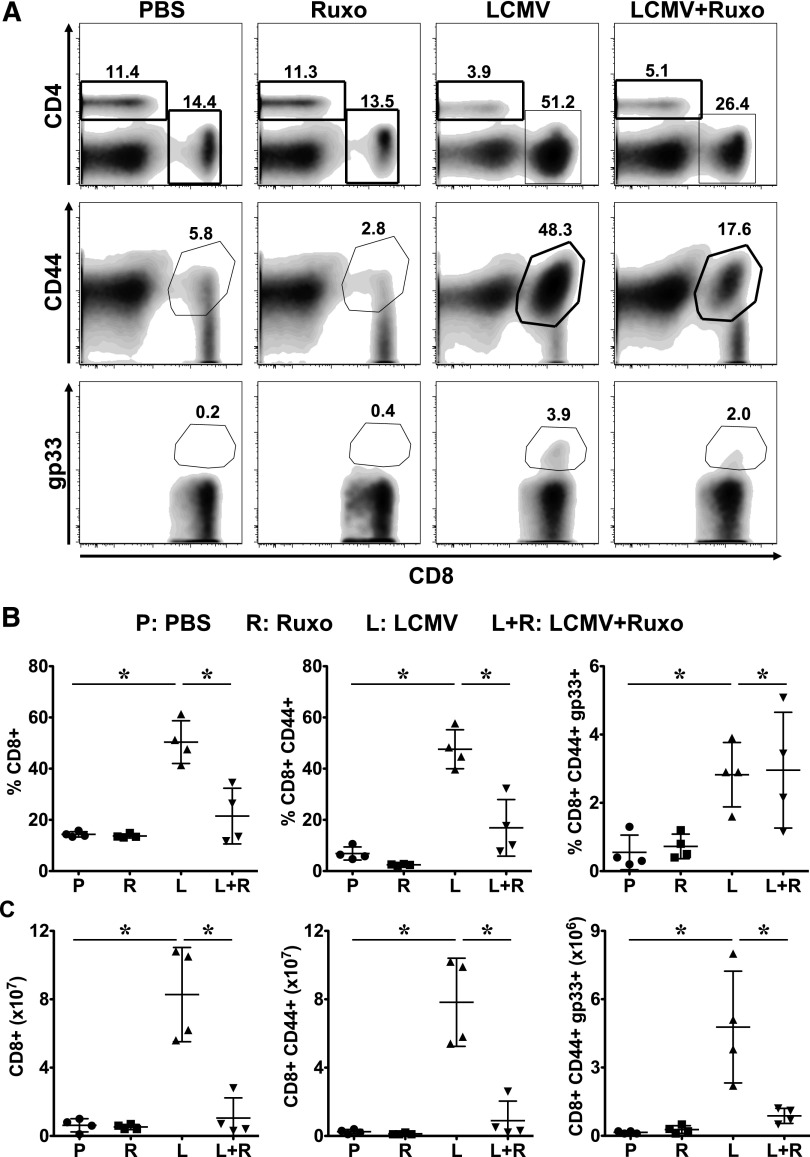
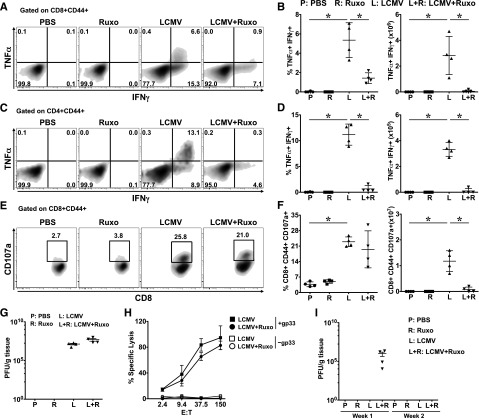
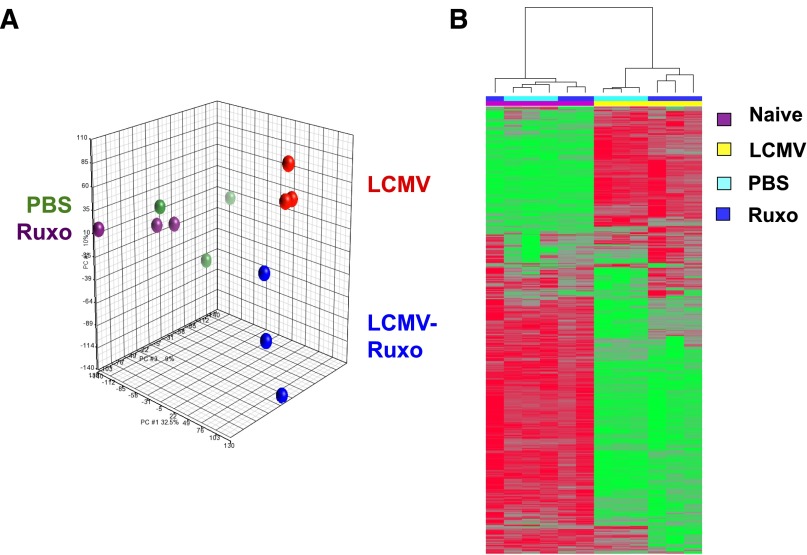
Hemophagocytic lymphohistiocytosis (HLH) comprises an emerging spectrum of inherited and noninherited disorders of the immune system characterized by the excessive production of cytokines, including interferon-γ and interleukins 2, 6, and 10 (IL-2, IL-6, and IL-10). The Janus kinases (JAKs) transduce signals initiated following engagement of specific receptors that bind a broad array of cytokines, including those overproduced in HLH. Based on the central role for cytokines in the pathogenesis of HLH, we sought to examine whether the inhibition of JAK function might lessen inflammation in murine models of the disease. Toward this end, we examined the effects of JAK inhibition using a model of primary (inherited) HLH in which perforin-deficient (Prf1(-∕-)) mice are infected with lymphocytic choriomeningitis virus (LCMV) and secondary (noninherited) HLH in which C57BL/6 mice receive repeated injections of CpG DNA. In both models, treatment with the JAK1/2 inhibitor ruxolitinib significantly lessened the clinical and laboratory manifestations of HLH, including weight loss, organomegaly, anemia, thrombocytopenia, hypercytokinemia, and tissue inflammation. Importantly, ruxolitinib treatment also significantly improved the survival of LCMV-infectedPrf1(-∕-)mice. Mechanistic studies revealed that in vivo exposure to ruxolitinib inhibited signal transducer and activation of transcription 1-dependent gene expression, limited CD8(+)T-cell expansion, and greatly reduced proinflammatory cytokine production, without effecting degranulation and cytotoxic function. Collectively, these findings highlight the JAKs as novel, druggable targets for mitigating the cytokine-driven hyperinflammation that occurs in HLH. These observations also support the incorporation of JAK inhibitors such as ruxolitinib into future clinical trials for patients with these life-threatening disorders.
© 2016 by The American Society of Hematology.
Figures
Comment in
-
Alleviating the storm: ruxolitinib in HLH.Blood. 2016 Mar 31;127(13):1626-7. doi: 10.1182/blood-2016-02-697151. Blood. 2016. PMID: 27034417
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
