

Application of Ultrasound-Guided Core Biopsy to Minimal-Invasively Diagnose Supraclavicular Fossa Tumors and Minimize the Requirement of Invasive Diagnostic Surgery
- PMID: 26825877
- PMCID: PMC5291547
- DOI: 10.1097/MD.0000000000002172
Application of Ultrasound-Guided Core Biopsy to Minimal-Invasively Diagnose Supraclavicular Fossa Tumors and Minimize the Requirement of Invasive Diagnostic Surgery
Abstract
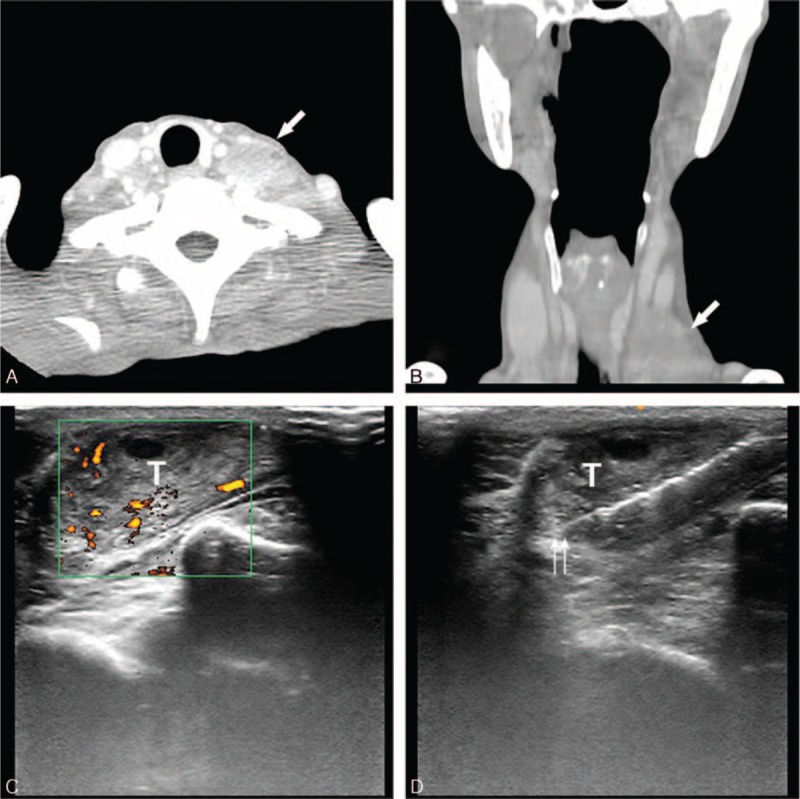
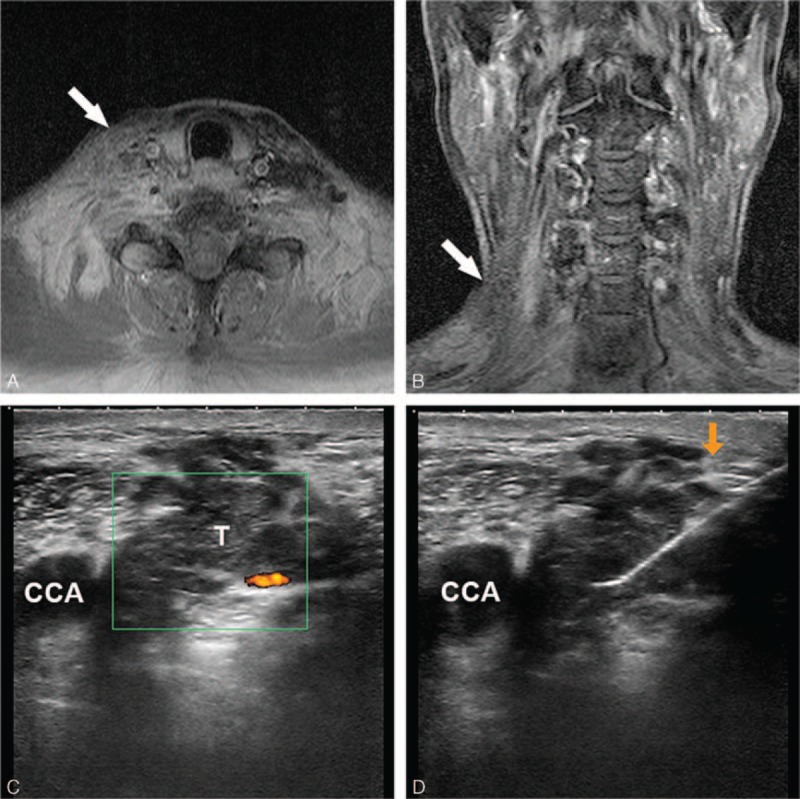
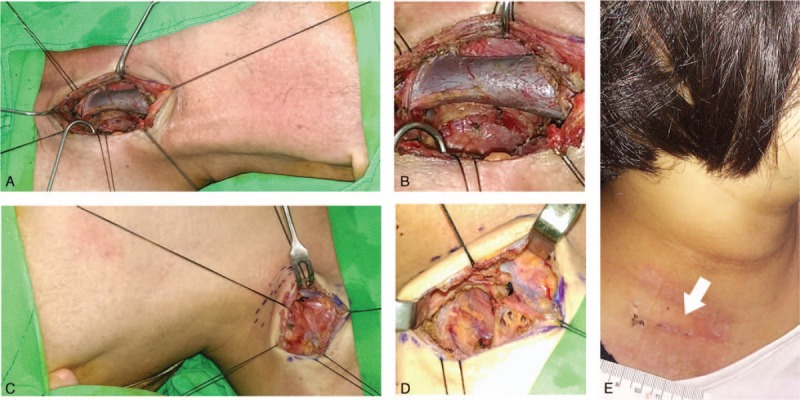
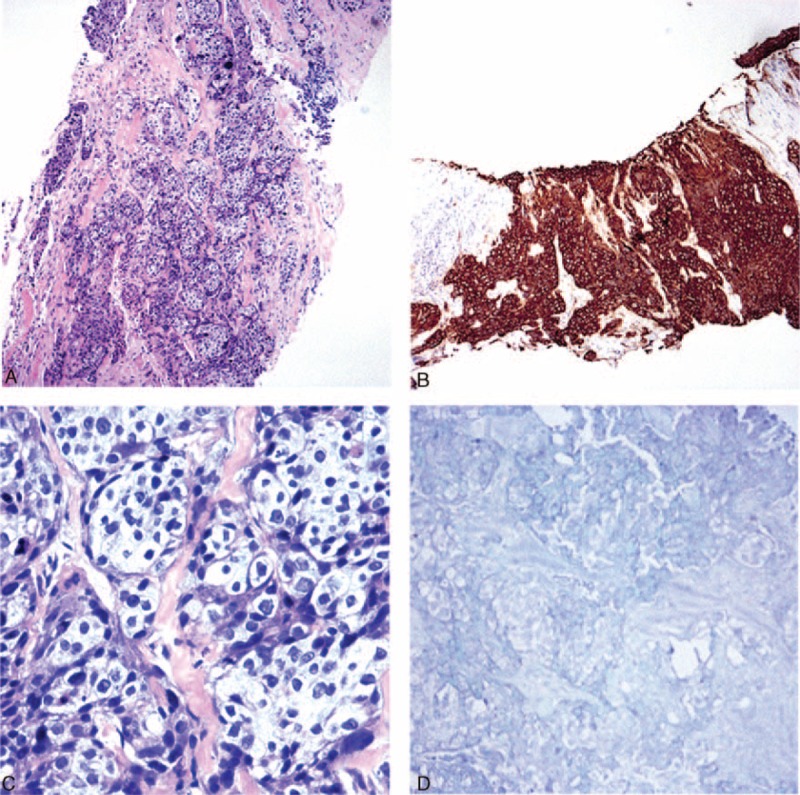
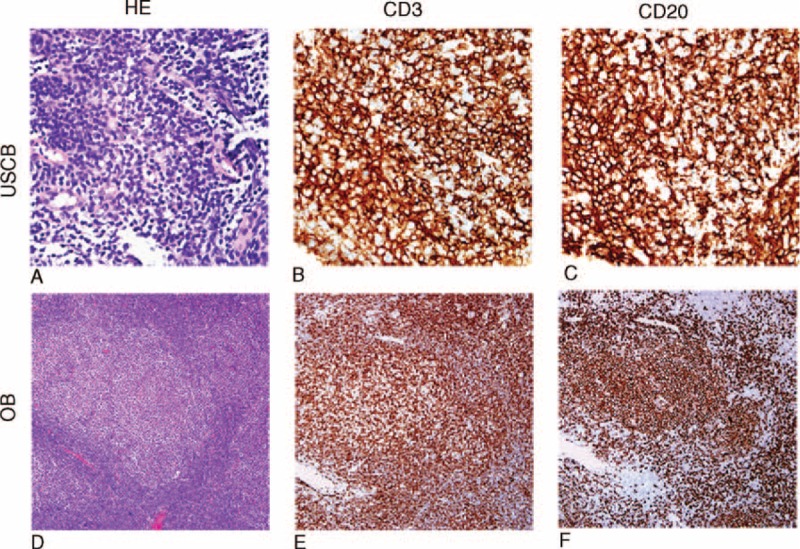
Tumors of the supraclavicular fossa (SC) is clinically challenging because of anatomical complexity and tumor pathological diversity. Because of varied diseases entities and treatment choices of SC tumors, making the accurate decision among numerous differential diagnoses is imperative. Sampling by open biopsy (OB) remains the standard procedure for pathological confirmation. However, complicated anatomical structures of SC always render surgical intervention difficult to perform. Ultrasound-guided core biopsy (USCB) is a minimally invasive and office-based procedure for tissue sampling widely applied in many diseases of head and neck. This study aims to evaluate the clinical efficacy and utility of using USCB as the sampling method of SC tumors. From 2009 to 2014, consecutive patients who presented clinical symptoms and signs of supraclavicular tumors and were scheduled to receive sampling procedures for diagnostic confirmation were recruited. The patients received USCB or OB respectively in the initial tissue sampling. The accurate diagnostic rate based on pathological results was 90.2% for USCB, and 93.6% for OB. No significant difference was noted between USCB and OB groups in terms of diagnostic accuracy and the percentage of inadequate specimens. All cases in the USCB group had the sampling procedure completed within 10 minutes, but not in the OB group. No scars larger than 1 cm were found in USCB. Only patients in the OB groups had the need to receive general anesthesia and hospitalization and had scars postoperatively. Accordingly, USCB can serve as the first-line sampling tool for SC tumors with high diagnostic accuracy, minimal invasiveness, and low medical cost.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures


Similar articles
-
Application of ultrasound-guided core biopsy to minimize the non-diagnostic results and the requirement of diagnostic surgery in extrapulmonary tuberculosis of the head and neck.Eur Radiol. 2016 Sep;26(9):2999-3005. doi: 10.1007/s00330-015-4159-4. Epub 2016 Jan 8. Eur Radiol. 2016. PMID: 26747256
-
Diagnosis of Kikuchi-Fujimoto disease: a comparison between open biopsy and minimally invasive ultrasound-guided core biopsy.PLoS One. 2014 May 2;9(5):e95886. doi: 10.1371/journal.pone.0095886. eCollection 2014. PLoS One. 2014. PMID: 24787483 Free PMC article.
-
The efficacy of incorporating ultrasound-guided core biopsy into the clinical workflow of indeterminate thyroid tumors.J Formos Med Assoc. 2022 Oct;121(10):2012-2019. doi: 10.1016/j.jfma.2022.02.003. Epub 2022 Feb 28. J Formos Med Assoc. 2022. PMID: 35241347
-
Ultrasound-guided core biopsy in the diagnosis of parotid neoplasia: an overview and update with a review of the literature.Br J Radiol. 2022 Feb 1;95(1130):20210972. doi: 10.1259/bjr.20210972. Epub 2021 Dec 3. Br J Radiol. 2022. PMID: 34860569 Free PMC article. Review.
-
Evaluation: Fine Needle Aspiration Cytology, Ultrasound-Guided Core Biopsy and Open Biopsy Techniques.Adv Otorhinolaryngol. 2016;78:39-45. doi: 10.1159/000442123. Epub 2016 Apr 12. Adv Otorhinolaryngol. 2016. PMID: 27093205 Review.
Cited by
-
The application of ultrasound in detecting lymph nodal recurrence in the treated neck of head and neck cancer patients.Sci Rep. 2017 Jun 21;7(1):3958. doi: 10.1038/s41598-017-04039-3. Sci Rep. 2017. PMID: 28638103 Free PMC article.
-
Histology-based and cytology-based needle sampling for targeted next-generation sequencing in the indeterminate thyroid tumors.Eur Arch Otorhinolaryngol. 2023 Aug;280(8):3773-3781. doi: 10.1007/s00405-023-07947-5. Epub 2023 Apr 25. Eur Arch Otorhinolaryngol. 2023. PMID: 37097467
References
-
- Gupta RK, Naran S, Lallu S, et al. The diagnostic value of fine needle aspiration cytology (FNAC) in the assessment of palpable supraclavicular lymph nodes: a study of 218 cases. Cytopathology 2003; 14:201–207. - PubMed
-
- Gupta N, Rajwanshi A, Srinivasan R, et al. Pathology of supraclavicular lymphadenopathy in Chandigarh, north India: an audit of 200 cases diagnosed by needle aspiration. Cytopathology 2006; 17:94–96. - PubMed
-
- Moberly AC, Vural E, Nahas B, et al. Ultrasound-guided needle aspiration: impact of immediate cytologic review. Laryngoscope 2010; 120:1979–1984. - PubMed
-
- Pfeiffer J, Kayser L, Ridder GJ. Minimal-invasive core needle biopsy of head and neck malignancies: clinical evaluation for radiation oncology. Radiother Oncol 2009; 90:202–207. - PubMed
-
- Chen CN, Yang TL. Application of ultrasound-guided core biopsy in head and neck. J Med Ultrasound 2014; 22:133–139.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
