

Safety and Efficacy of EUS-Guided Ethanol Ablation for Treating Small Solid Pancreatic Neoplasm
- PMID: 26825894
- PMCID: PMC5291564
- DOI: 10.1097/MD.0000000000002538
Safety and Efficacy of EUS-Guided Ethanol Ablation for Treating Small Solid Pancreatic Neoplasm
Abstract
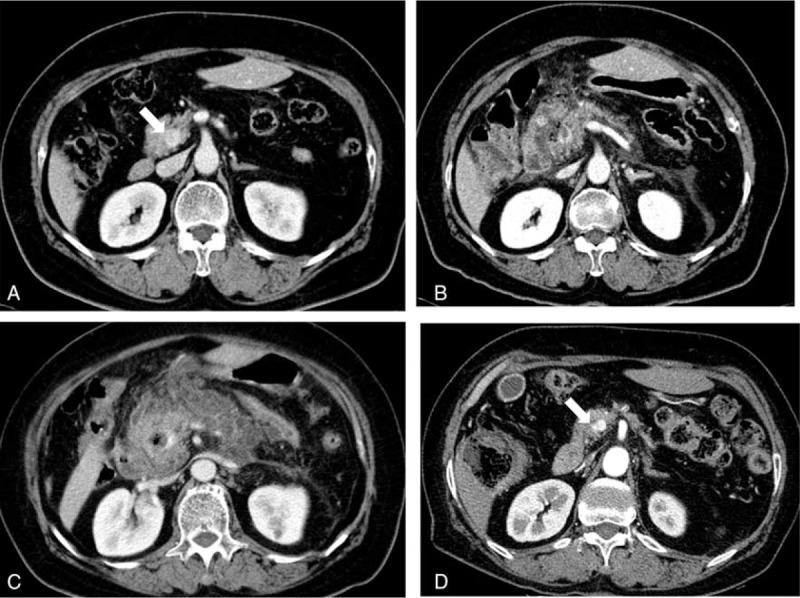
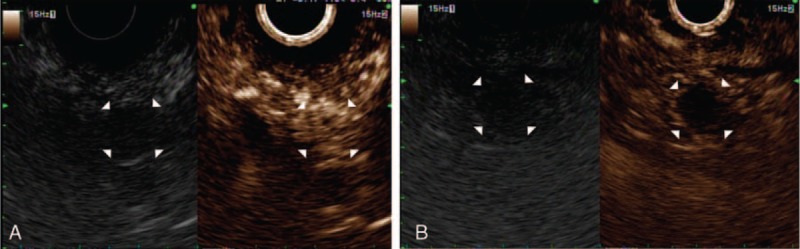
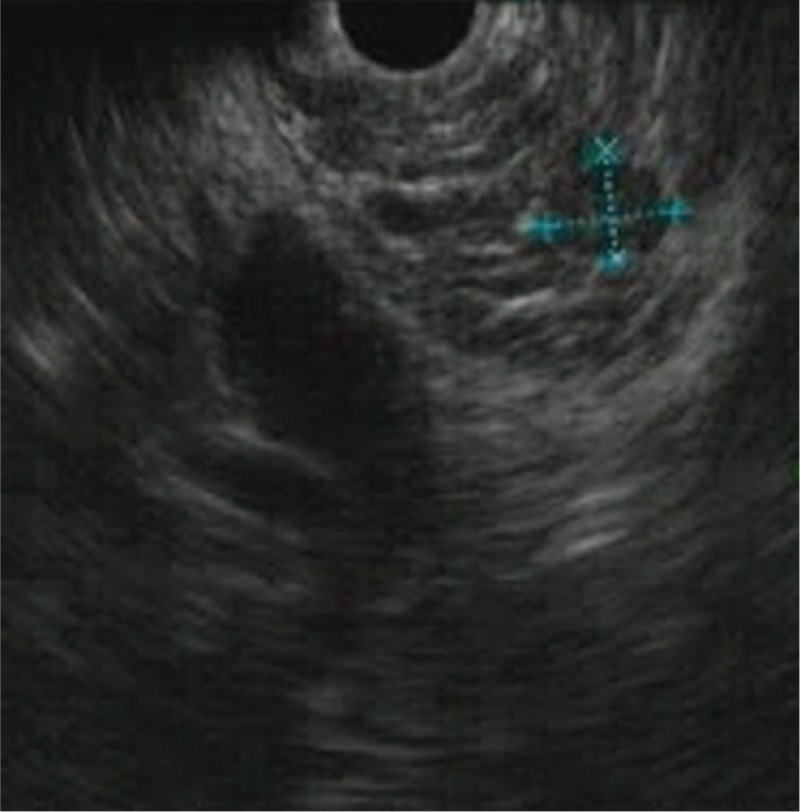
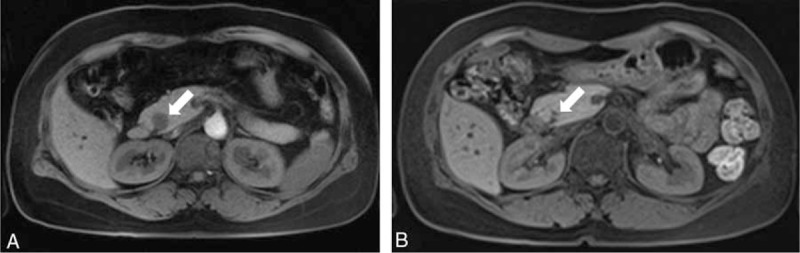
The strategy for treating small borderline malignant pancreatic neoplasms--such as neuroendocrine tumor (NET) and solid pseudopapillary neoplasm (SPN)--is surgical resection. However, pancreatic resection of these lesions still causes significant morbidity. We evaluated the safety and efficacy of EUS-guided ethanol ablation to treat small solid pancreatic neoplasms. A total of 8 patients with small borderline malignant pancreatic neoplasms and co-morbidities who refused surgery were included. We identified 2 cases of nonfunctioning NET, 3 cases of insulinomas, 1 case of gastrinoma, and 2 cases of SPN. EUS-guided ethanol ablation was performed, and treatment outcomes were assessed with clinical symptom, hormone assay, and imaging study. The mean tumor diameter was 15 mm (range, 7-29 mm), and the median volume of injected ethanol was 2.8 mL (range, 1.2-10.5 mL). There was 1 severe acute pancreatitis after EUS-guided ethanol ablation with 20-gauge CPN needle. During follow-up (median 16.5 months), 6 patients achieved treatment success; however, 2 patients (1 nonfunctioning NET and 1 SPN) still had persistent tumors. The patient with persistent SPN underwent surgical resection and the histopathological results showed peripancreatic infiltration with perineural invasion. Among 6 patients who achieved initial treatment success, 1 patient experienced tumor recurrence within 15 months and underwent repeated EUS-guided ethanol ablation. In conclusion, EUS-guided ethanol ablation therapy is a promising option for patients with small solid pancreatic neoplasm. Multiple sessions or surgical interventions may be required if there is a recurrent or persistent mass, and procedure-related adverse events must be carefully monitored.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
-
- Cheema A, Weber J, Strosberg JR. Incidental detection of pancreatic neuroendocrine tumors: an analysis of incidence and outcomes. Ann Surg Oncol 2012; 19:2932–2936. - PubMed
-
- Gaujoux S, Partelli S, Maire F, et al. Observational study of natural history of small sporadic nonfunctioning pancreatic neuroendocrine tumors. J Clin Endocrinol Metab 2013; 98:4784–4789. - PubMed
-
- Santini D, Poli F, Lega S. Solid-papillary tumors of the pancreas: histopathology. JOP 2006; 7:131–136. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
